La spécificité du tadalafil est liée à sa longue demi-vie, permettant une action qui excède largement celle des autres inhibiteurs de PDE5. L’absorption digestive est complète, avec un pic plasmatique atteint en 2 heures environ. Le métabolisme est réalisé via CYP3A4, produisant des métabolites inactifs éliminés principalement dans les fèces. La sélectivité enzymatique est élevée, réduisant les effets indésirables extra-caverneux. Les réactions indésirables fréquentes incluent céphalées, bouffées vasomotrices et troubles digestifs légers. L’activité pharmacologique est stable, indépendamment de l’ingestion d’aliments. Dans les comparaisons de longue durée, acheter cialis pas cher est mentionné en relation avec les études portant sur la persistance d’efficacité et la constance de la cinétique plasmatique.
11cu.wallner
Verrucous Porokeratosis of Mibelli on the Buttocks Mimicking PsoriasisJuliann S. Wallner, MD; James E. Fitzpatrick, MD; Sylvia L. Brice, MD
T h e t y p i c a l p re s e n t a t i o n o f p o ro k e r a t o s i s o f
small keratotic papules and enlarge centrifugally to
Mibelli is of a solitar y plaque with a prominent
form annular or serpiginous lesions, ranging from a
raised border cleaved by a central furrow. The
few millimeters to several centimeters in diameter. central por tion of the plaque is usually slightly
Lesions are usually asymptomatic but can be pru-
atrophic. The plaques var y in size from a few mil-
ritic. Although onset can occur at any age, poro-
limeters to several centimeters in diameter and
keratosis usually appears during childhood. Sporadic
tend to be acrally distributed, though they can
cases, however, generally occur later in life. Men
occur on any par t of the body. We repor t anu n u s u a l c a s e o f v e r r u c o u s p o ro k e r a t o s i s o f
Lucker et al1 and Stone et al2 both described
Mibelli, localized to the natal cleft, that mimicked
individual cases of a verrucous type of porokerato-
psoriasis. This entity, though unusual, is not
sis of Mibelli that was localized to the natal cleft
unique. Two similar cases of verrucous poroker-
region. We report a similar case of verrucous poro-
atosis of Mibelli limited to the natal cleft region
keratosis of Mibelli limited to the natal cleft that
and resembling psoriasis have been repor ted inthe British literature. Verrucous porokeratosis ofMibelli localized to the natal cleft appears to beCase Report a distinct clinical entity that can mimic psoriasis.
A 44-year-old Asian man presented with a 28-year
Better recognition of this for m of porokeratosis of
history of pruritic plaques on the buttocks. These
Mibelli may result in earlier diagnosis and initia-
plaques had been gradually enlarging. The patient
had seen several dermatologists and undergone
various treatments for psoriasis, including topicalsteroids, coal tar, calcipotriene, tazarotene, psoralen-UVA, and topical tacrolimus, all of which were
Porokeratosis is a heterogeneous group of dis- unsuccessful. He had a history of essential hyper-
orders inherited in an autosomal-dominant
tension and glaucoma but was otherwise healthy.
fashion and characterized histologically by the
His medications included losartan, hydrochloro-
presence of a cornoid lamella. The plaque type,
thiazide, triamterene, and brimonidine eyedrops.
termed porokeratosis of Mibelli, has a predilection
Family history of skin disease included only atopic
for the acral areas and perigenital region. Poroker-
dermatitis. Results from a review of systems were
atosis of Mibelli is characterized clinically by one
or more plaques, with a prominent raised border
On physical examination, several well-demarcated,
cleaved by a central furrow. The center of the
scaly, red-brown, verrucous plaques with hyper-
plaque is often atrophic, hairless, and either hyper-
pigmented raised borders distributed bilaterally on
pigmented or hypopigmented. However, lesions
the buttocks (Figure 1) were noted. No other cuta-
can be psoriasiform or verrucous, with varying
neous lesions were evident, and there was no
degrees of hyperkeratosis. The lesions begin as
Two biopsies were obtained. The first, a 4-mm
Accepted for publication May 8, 2003.
punch biopsy of the center of a plaque, demon-
From the Department of Dermatology, University of Colorado
strated psoriasiform hyperplasia of the epidermis
with focal parakeratosis suggestive of a cornoid
The authors report no conflict of interest.
lamella. The second, a 6-mm punch biopsy of the
Reprints: Sylvia L. Brice, MD, Department of Dermatology,
border of a plaque, revealed a thin column of
University of Colorado Health Sciences Center, Anchutz CancerPavilion, PO Box 6510, Mail Stop F703, Aurora, CO 80010
parakeratotic cells with underlying absence of the
granular layer and dyskeratotic and vacuolated
Figure 1. Scaly verrucous plaques with hyperpig- mented raised borders on the buttocks.
cells in the spinous layer, which is characteristic of
34-year-old man with a 9-year history of pruritic
a cornoid lamella (Figure 2). Although there was
dermatosis confined to the natal cleft. They deter-
some psoriasiform hyperplasia, the rete ridges were
mined this to be a novel form of porokeratosis,
not club shaped, and no thinning of the suprapap-
which they termed porokeratosis ptychotropica from
illary plate or platelike parakeratosis and no collec-
the Greek words ptyché (fold) and tropé (a turning).
tions of neutrophils in the epidermis or stratum
In 1999, Stone et al2 described a 32-year-old man
corneum were noted, as seen in psoriasis. This was
with a 13-year history of pruritic dermatosis con-
consistent with porokeratosis, making the diag-
fined to the natal cleft, which they termed verrucousporokeratosis. As with our case, this second case also
The patient underwent a trial of imiquimod
had been mistaken for and treated as psoriasis. All
cream applied once a day to one side of the but-
3 cases presented in young men and were intensely
tocks and 5-fluorouracil cream applied twice a day
pruritic, progressive, and confined to the natal cleft.
to the other side. The imiquimod cream caused
As suggested in the previous case reports, this may
severe irritation without much improvement and
represent a distinct clinical variant of porokeratosis.
was discontinued. Subsequently, the 5-fluorouracil
Porokeratosis is known to undergo malignant
cream was applied to the entire lesion for transformation to Bowen disease, squamous cell 2 months, with resolution of the scaling and pruri-
carcinoma, and basal cell carcinoma; the latest
tus but with no decrease in the verrucous compo-
review revealed at least 56 published cases.8 This
nent or size of the plaques. After this therapy,
review found that approximately 11% of patients
treatment consisted of a trial of carbon dioxide
with porokeratosis have lesions that undergo malig-
(CO ) laser resurfacing on one side and dermabrasion
nant transformation. Malignant transformation in
on the other side. The porokeratosis recurred on porokeratosis has been associated with an over-the side treated with CO laser resurfacing. How-
expression of p53.9-11 This potential for malignant
ever, dermabrasion successfully removed the poro-
transformation makes distinguishing porokeratosis
keratosis, and, at the 6-month follow-up, no clinical
evidence of porokeratosis in the dermabrasion-
Treatment of porokeratosis has been largely
anecdotal. There are isolated case reports of successful treatment using topical 5-fluorouracil
(with and without occlusion), isotretinoin and
Porokeratosis of Mibelli localized to the genital
region alone is rare, with only 7 reported cases.1-7
dye laser radiation, grenz ray radiation, frequency-
Two of these cases are clinically and histologically
doubled Q-switched Nd:YAG laser radiation,
identical to ours. In 1995, Lucker et al1 described a
cryotherapy, dermabrasion, surgical excision, and
Figure 2. Cornoid lamella formation with the charac- teristic slanted column of coarse parakeratosis and underlying loss of the granular layer (H&E, original magnification ϫ60).
electrodesiccation. In this case, topical 5-fluorouracil,
3. Levell NJ, Bewley AP, Levene GM. Porokeratosis of
imiquimod cream, and CO laser resurfacing were
Mibelli on the penis, scrotum and natal cleft. Clin Exp
all ineffective in clearing the porokeratosis. How-
ever, we found dermabrasion to be a potentially
4. Neri I, Marzaduri S, Passarini B, et al. Genital poroker-
long-term and effective treatment for porokeratosis
atosis of Mibelli. Genitourin Med. 1995;71:410-411.
5. Tangoren I, Weinberg JM, Ioffreda M, et al. Penile
In summary, verrucous porokeratosis limited to
porokeratosis of Mibelli. J Am Acad Dermatol.
the natal cleft appears to be a distinct clinical entity
that may mimic localized psoriasis. Some of the
6. Trcka J, Pettke-Rank C, Brocker EB, et al. Genitoanocrural
treatment modalities used for psoriasis are inappro-
porokeratosis following chronic exposure to benzene. Clin
priate and ineffective for porokeratosis (eg, UV
light). However, unlike psoriasis, verrucous lesions
7. Robinson JB, Im DD, Jockle G, et al. Vulvar porokeratosis:
of porokeratosis should be monitored for malignant
case report and review of the literature. Int J Gynecol Pathol.
change because correct diagnosis is important for
optimal patient care. This stresses the importance of
8. Otsuka F, Someya T, Ishibashi Y. Porokeratosis and malig-
considering a biopsy in cases where the skin disease
nant skin tumors. J Cancer Res Clin Oncol. 1991;117:55-60.
is not responsive to appropriate therapy.
9. Magee JW, McCalmont TH, LeBoit PE. Overexpression
of p53 tumor suppressor protein in porokeratosis. ArchDermatol. 1994;130:187-190. REFERENCES
10. Puig L, Alegre M, Costa I, et al. Overexpression of p53 in dis-
1. Lucker GP, Happle R, Steijlen PM. An unusual case of
seminated superficial actinic porokeratosis with and without
porokeratosis involving the natal cleft: porokeratosis
malignant degeneration. Arch Dermatol. 1995;131:353-354.
ptychotropica? Br J Dermatol. 1995;132:150-151.
11. Sasaki S, Urano Y, Nakagawa K, et al. Linear porokerato-
2. Stone N, Ratnavel R, Wilkinson JD. Bilateral perianal
sis with multiple squamous cell carcinomas: study of p53
inflammatory verrucous porokeratosis (porokeratosis
expression in porokeratosis and squamous cell carcino-
ptychotropica). Br J Dermatol. 1999;140:553-555.
mas. Br J Dermatol. 1996;134:1151-1153.
New Technology Offers New Opportunities: Continuous Bronchodilator Therapy Key words: aerosol, ventilator, nebulizer, pMDI, DPI Mr. Fink was previously an employee of Aerogen, Inc., and involved in the development of the Aeroneb vibrating mesh technology and its use in critical care Introduction Patients with severe exacerbations of asthma, refractory to standard dose and frequency of inh
Pharmaceutical Product Manufacturing in Indonesia Copyright & Disclaimer This product has been supplied by PT. Dataindo Inti Swakarsa ('DIS-IBISWorld') solely for use by its authorised licensees strictly in accordance with their license agreements with DIS-IBISWorld. DIS-IBISWorld makes no representation to any other person with regard to the completeness or accuracy of the data or in
 Figure 1. Scaly verrucous
Figure 1. Scaly verrucous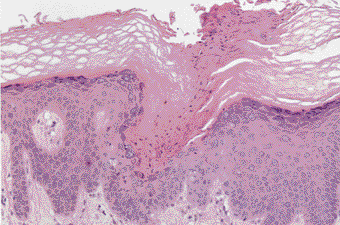 Figure 2. Cornoid lamella
Figure 2. Cornoid lamella