La spécificité du tadalafil est liée à sa longue demi-vie, permettant une action qui excède largement celle des autres inhibiteurs de PDE5. L’absorption digestive est complète, avec un pic plasmatique atteint en 2 heures environ. Le métabolisme est réalisé via CYP3A4, produisant des métabolites inactifs éliminés principalement dans les fèces. La sélectivité enzymatique est élevée, réduisant les effets indésirables extra-caverneux. Les réactions indésirables fréquentes incluent céphalées, bouffées vasomotrices et troubles digestifs légers. L’activité pharmacologique est stable, indépendamment de l’ingestion d’aliments. Dans les comparaisons de longue durée, acheter cialis pas cher est mentionné en relation avec les études portant sur la persistance d’efficacité et la constance de la cinétique plasmatique.
Cognitive improvement following treatment in late-life depression: relationship to vascular risk and age of onset
Cognitive Improvement Following Treatment in Late-Life Depression: Relationship to Vascular Risk and Age Deanna M. Barch, Ph.D., Gina D’Angelo, Ph.D., Carl Pieper, Dr.P.H, Consuelo H. Wilkins, M.D., Kathleen Welsh-Bohmer, Ph.D., Warren Taylor, M.D., Keith S. Garcia, M.D., Kenneth Gersing, M.D., P. Murali Doraiswamy, M.D., Yvette I. Sheline, M.D. Objectives: To test the hypothesis that the degree of vascular burden and/or age of onset may influence the degree to which cognition can improve during the course of treatment in late-life depression. Design: Measurement of cognition both before and following 12 weeks of treatment with sertraline. Setting: University medical centers (Washington University and Duke University). Participants: One hundred sixty-six individuals with late-life depression. Intervention: Sertraline treatment. Measurements: The cognitive tasks were grouped into five domains (language, pro- cessing speed, working memory, episodic memory, and executive function). We mea- sured vascular risk using the Framingham Stroke Risk Profile measure. We mea- sured T2-based white matter hyperintensities using the Fazekas criteria. Results: Both episodic memory and executive function demonstrated significant improvement among adults with late-life depression during treatment with sertraline. Importantly, older age, higher vascular risk scores, and lower baseline Mini-Mental State Exami- nation scores predicted less change in working memory. Furthermore, older age, later age of onset, and higher vascular risk scores predicted less change in executive func- tion. Conclusions: These results have important clinical implications in that they suggest that a regular assessment of vascular risk in older adults with depression is necessary as a component of treatment planning and in predicting prognosis, both for the course of the depression itself and for the cognitive impairments that often accompany depression in later life. (Am J Geriatr Psychiatry 2012; 20:682–690) Key Words: Cognition, treatment, vascular depression, white matter
Received November 11, 2010; revised February 25, 2011; accepted April 08, 2011. From the Departments of Psychology (DMB), Psychiatry(DMB, CHW, KSG, YJS), Radiology (DMB, YJS), and Division of Biostatistics (GD’A), Washington University School of Medicine, St. Louis,MO; and Department of Psychiatry, Duke University School of Medicine, Durham, NC (CP, KW-B, WT, KG, PMD). Send correspondenceand reprint requests to Deanna M. Barch, Ph.D., Departments of Psychology, Psychiatry, and Radiology, Washington University, Box 1125,One Brookings Dr, St. Louis, MO 63130. e-mail: [email protected]
Supplemental digital content is available for this article. Direct URL citations appear in the printed text and are provided in the HTML
and PDF versions of this article on the journal’s Web site (www.AJGPonline.org).
C 2012 American Association for Geriatric Psychiatry
Am J Geriatr Psychiatry 20:8, August 2012
Copyright American Association for Geriatric Psychiatry. Unauthorized reproduction of this
Numerous studies document the presence of Such findings in younger adults raise the possi-
a range of cognitive impairments in late-life
bility that at least some aspects of cognitive dys-
depression,1,2 including reductions in working mem-
function in late-life depression may not necessarily
ory, executive function, episodic memory, and pro-
result from accruing vascular changes but may reflect
cessing speed.1,2 One hypothesis is that the presence
state or even trait aspects of depression. If so, one
of such cognitive impairments in late-life depression
might expect more robust evidence for improvement
reflects frontal striatal and/or hippocampal dysfunc-
in cognitive function across the course of treatment
tion that may result—at least in part—from vascu-
in late-life depression. Several studies have found
lar disease,3–6 and that this may be particularly true
some evidence for such improvement, with the mag-
for depression with a later age of onset. Given this
nitude of improvement in cognitive function corre-
hypothesis, it is not surprising that cognitive impair-
lated with the magnitude of improvement in depres-
ment persists following depression treatment in older
sion in some studies.19–25 However, a number of other
adults (for a review, see Douglas and Porter7). As such,
studies have either found no improvement in cogni-
the goal of this article was to examine the influence of
tion as a function of treatment in late-life depression
vascular risk and age of onset on cognitive improve-
or that the level of cognitive function in antidepres-
ment following depression treatment in older adults.
sant responders was still below that of individuals
that more severe cognitive impairment among older
One important factor that these studies have not
adults with depression predicts poorer outcome8,9
taken into account is the role that vascular burden
and a poorer response to treatment.10–13 Furthermore,
and the presence of white matter hyperinstensities
older adults with greater evidence of white matter
may play in moderating cognitive change. Some stud-
impairment13,14 or reduced hippocampal and cor-
ies have found that older adults with depression are
tical volumes15,16 also show a poorer response to
either less likely to respond to antidepressant treat-
treatment. All of these results are consistent with
ment or slower to respond.31 This could reflect the
the hypotheses that cognitive impairments in late-
influence of vascular changes and white matter alter-
life depression result from vascular or other neural
ations in older adults with depression. If so, then the
changes that contribute to the onset or recurrence of
degree vascular burden, white matter hyperintensi-
depression in late life and are not transient or state-
ties, and/or age of onset may influence the degree
related manifestations of the presence of depression. If
to which cognition can improve during treatment in
so, it is not surprising that such cognitive deficits per-
late-life depression. The goal of this study was to test
sist even among individuals who respond to depres-
these hypotheses by examining the degree to which
vascular risk, white matter hyperintensities, and age
However, there is also evidence that cognitive
of onset predict the degree of cognitive improvement
impairments are present in depression with an ini-
during 12 weeks of sertraline treatment in a large sam-
tial onset in young adulthood or middle age. These
ple of older adults with Diagnostic and Statistical Man-
deficits are often present in many of the same cog-
ual of Mental Disorders, Fourth Edition (DSM-IV), Major
nitive domains impaired in late-life depression,17
though the robustness of such cognitive impair-ments in early or midlife adult depression has beenmixed across studies.18 Furthermore, there is evi-
dence that at least some of these cognitive impair-
Participants
ments can improve during treatment in youngerdepressed adults. Specifically, Douglas and Porter7
Participants were recruited as part of a National
recently reviewed this literature and concluded that
Institute of Mental Health–funded study through
measures of episodic memory, verbal fluency, and
advertising and physician referral to Washington Uni-
processing speed varied as a function of clinical state
versity (WU) and Duke University (Duke). Patients
in depression, with deficits in executive function and
were recruited into the study if they met DSM-IV cri-
attention showing more stable and trait-like charac-
teria for MDD by Structured Clinical Interview for
teristics in younger adults with depression.
Axis I DSM-IV Disorders (SCID-IV),32 administered
Am J Geriatr Psychiatry 20:8, August 2012
Copyright American Association for Geriatric Psychiatry. Unauthorized reproduction of this
Cognitive Change in Late-Life Depression
by a research psychiatrist, and were 60 years or older.
(MADRS).35 The MADRS was administered by a
Exclusion criteria included 1) severe or unstable medi-
research psychiatrist at the start of the trial and
cal disorders; 2) known primary neurologic disorders;
during each week of the trial. We assessed overall
3) history of other Axis I disorders prior to the depres-
cardiovascular risk using the Framingham Stroke
sion diagnosed by SCID-IV; 4) current suicidal risk; 5)
Risk Profile.36 The Framingham Stroke Risk Profile
a current MDD episode that had failed to respond to
generates a composite score using the following
adequate trials of two prior antidepressants for at least
vascular risk factors to predict 10-year probability
6 weeks at therapeutic doses; 6) use of psychotropic
of stroke in both men and women: age, systolic
prescription or nonprescription drugs or herbals (e.g.,
blood pressure, the use of antihypertensive therapy,
Hypericum) within 3 weeks or 5 half-lives; 7) inpatient
diabetes mellitus, cigarette smoking, cardiovascular
status; or 8) Clinical Dementia Rating greater than 0 or
disease (coronary heart disease, cardiac failure, or
Mini-Mental State Examination score less than 21.27 Of
intermittent claudication), atrial fibrillation, and
362 phone screens at WU and 374 at Duke, there were
left ventricular hypertrophy by electrocardiogram.
181 clinic screens at WU and 135 at Duke (for details,
This score has been positively associated with white
see Sheline et al.13). The 316 clinic screens resulted in
matter hyperintensities37 and negatively associated
217 participants (120 at WU and 97 at Duke) being
with total brain volume.38 We also assessed baseline
enrolled in a 12-week treatment trial with sertraline.
global cognitive function using the Clinical Dementia
Of these participants, 190 completed treatment (109
Rating39 and Mini-Mental State Examination.40 We
at WU and 81 at Duke). Written informed consent
assessed age at onset from the SCID-IV and all
approved by the relevant institutional review board
available medical and psychiatric records.
was obtained for all subjects. This trial is registeredat clinical trials.gov Treatment Outcome of Vascular
Neuropsychological Function
Participants were administered a large battery
Sertraline Treatment
of neuropsychological tests that covered cognitivedomains relevant to understanding late-life depres-
Sertraline was selected as the SSRI in this
sion at both baseline (prior to the start of medications)
study because it is among the more selective
and at the end of the 12 weeks of treatment. The neu-
5-hydroxytryptamine (5-HT; also serotonin) re-
ropsychological testing was performed by a trained
uptake inhibitors, has an excellent profile for safety
examiner who was supervised by a Ph.D.-level psy-
and effectiveness in the treatment of MDD in the con-
chologist (DB and KWB). We grouped the cognitive
text of comorbid illness,33 has linear kinetics, and has
tasks into rationally motivated domains described
minimal age effect on clearance.34 The primary results
later, based on the prior literature regarding the cog-
of depression response to treatment have been previ-
nitive processes tapped by each of the tasks. The
ously reported.13 Briefly, the treatment consisted of
domains were executive function, processing speed,
an initial dose of sertraline at 25 mg for 1 day to rule
episodic memory, working memory, and language
out drug sensitivity and then 50 mg daily, with sub-
processing. To combine the tasks within each cog-
sequent dose changes at 2, 4, and 6 weeks (to 100,
nitive domain, we created Z-scores for the primary
150, and 200 mg per day, respectively). At any point,
dependent measure of interest using the scores from
patients who had side effects could be titrated to a
both baseline and follow-up across all participants
lower dose. Medication adherence was assessed on
and then summed the Z-scores (the results would not
each visit by self-report. At the end of treatment, the
have been different if only the baseline was used to
mean final dose was 114, with 64 on less than 100 mg,
create Z-scores). For the majority of variables, a higher
60 on 100 to 125 mg, 46 on 150 to 175 mg, and 34 on
score indicated better performance. We reverse scored
any items (e.g., reaction time on Trails B) for which
Measures
good performance was indicated by a lower value. Cronbach’s α (a measure of internal consistency) was
We assessed depression severity using the
computed for each domain from the baseline data.
For further details, see Sheline et al.,2 who describe
Am J Geriatr Psychiatry 20:8, August 2012
Copyright American Association for Geriatric Psychiatry. Unauthorized reproduction of this
the baseline analyses of neuropsychological function
School of Medicine by RCM and YIS. The modi-
fied Fazekas criteria35 describe magnetic resonance
Executive function. This domain included verbal
imaging hyperintensities in three regions (periven-
fluency (total phonological and semantic), Trails B
tricular, deep white matter, and subcortical gray mat-
(reverse scored time to completion), the color-word
ter regions), using ascending degree of severity. The
interference condition of the Stroop task (number
dependent variable was a total score summing sever-
completed), the Initiation-Perseveration subscales of
ity scores in all three regions. See Supplemental Digi-
the Mattis, and categories completed from the Wis-
tal Content 1 (http://links.lww.com/AJGP/A28) for
consin Card Sorting Test. The coefficient α for this
Processing speed. This domain included symbol-
digit modality (number completed), the color nam-ing condition of the Stroop task (number completed),
and Trails A (reverse scored time to completion). Thecoefficient α for this domain was 0.80.
Of the 217 individuals enrolled in the trial, 211 had
Episodic memory. This domain included word list
usable neuropsychological data at baseline. Of the 190
learning (total correct), logical memory (total correct
individuals who completed the trial, 166 (105/109 at
immediate), constructional praxis (Rey-Osterrieth
WU, 61/81 at Duke) were able to provide cognitive
Complex Figure Test memory performance), and the
data at the 12-week follow-up. We began by com-
Benton Visual Retention Test (total correct). The coef-
paring the demographic, clinical, and cognitive char-
ficient α for this domain was 0.76.
acteristics of the participants with usable neuropsy-
Language processing. This domain included the
chological data at baseline (n = 211) who did (n =
Shipley Vocabulary Test (number correct), the Boston
166) and did not have data at study completion.13 As
Naming Test (number correct), and the word reading
shown in Table 1, these two groups did not differ in
condition of the Stroop task (number completed). The
age, education, gender, race, baseline MADRS, base-
coefficient α for this domain was 0.67.
line Mini-Mental State Examination scores, vascular
Short-term/working memory. This domain included
risk, or on any of the 5 cognitive domains. The indi-
digit span forward (number of trials correctly com-
viduals who did not have neuropsychological data at
pleted), digit span backward (number of trials cor-
study completion had a slightly but significantly later
rectly completed), and ascending digits (number of
age of onset than those individuals who did not.
trials correctly completed). The coefficient α for thisdomain was 0.68. Did Cognition Improve Across the Course Magnetic Resonance Imaging of Treatment?
Both T1 and T2 magnetic resonance images were
To examine whether performance in any of the
collected using a Siemens Sonata 1.5-T scanner at
five cognitive domains improved across treatment,
WU School of Medicine and a GE 1.5-T scan-
we used a repeated-measures analysis of variance
ner at Duke. See Supplemental Digital Content 1
with time point (baseline, follow-up) and cognitive
(http://links.lww.com/AJGP/A28) for details on
domain (language, processing speed, working mem-
ory, episodic memory, executive function) as within-subject factors, and the domain Z-score as the depen-
T2-Weighted Hyperintensities
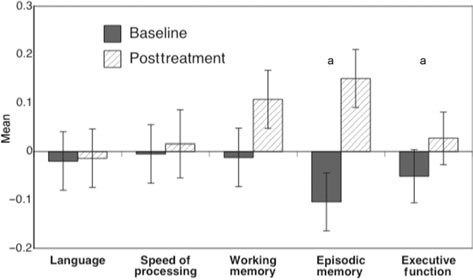
dent measure. This analysis revealed a main effect oftime, F(1,165) = 19.3, p <0.0001, and a time by cog-
Hyperintensities were assessed blinded to treat-
nitive domain interaction, F(4,660) = 11.1, p <0.001.
ment data using the modified Fazekas criteria, which
As shown in Figure 1, follow-up contrasts for each
are widely used measures of white matter burden
cognitive domain indicated that only episodic mem-
that allows comparison with a large number of pre-
ory and executive function improved over the course
vious studies. All ratings were conducted at WU
Am J Geriatr Psychiatry 20:8, August 2012
Copyright American Association for Geriatric Psychiatry. Unauthorized reproduction of this
Cognitive Change in Late-Life DepressionTABLE 1. Demographic, Clinical, and Cognitive Characteristics of Participants Mean (SD) Comparison of Completers and Variable Completers Noncompleters Noncompleters t(209) = 2.06, p = 0.04 Notes: bold value indicates the only variable that differed between completers and non-completers.
MMSE, Mini-Mental State Examination.
thus we used Spearman rank order correlations to
FIGURE 1. Graph of performance in each of the five cognitive domains at baseline and at
examine the relationship with cognitive change for
posttreatment. Significance of change in each
this variable. As shown in Table 2, older age pre-
cognitive domain was assessed with post-hoc
dicted less improvement in processing speed, work-
contrast (F-tests with 1,165 dfs).
ing memory, and executive function. Later age ofonset predicted less improvement in executive func-tion. Higher vascular risk predicted less change inworking memory and executive function. More severewhite matter hyperintensities predicted less change inprocessing speed. Of note, the results were essentiallyidentical when partial correlations were used, exam-ining the relationship between posttreatment perfor-mance and the predictors, covarying for baseline cog-nitive performance.
We also examined whether the magnitude of
improvement in depression predicted the magnitudeof improvement in cognition. To do so, we created
a residualized change score for depression usingbaseline MADRS scores to predict posttreatment
What Factors Predict Improved Cognition?
MADRS scores and correlated this with the residu-alized change scores for cognition. As shown in Table
We computed residualized change scores for each
2, a greater reduction in MADRS scores predicted a
of the five cognitive domains, using baseline perfor-
greater improvement in language function but did not
mance to predict posttreatment performance. We then
predict improvement in the other cognitive domains.
used Pearson’s product moment correlations to com-pute the correlations between age, age of onset, vascu-
Cognitive Improvement As a Function of
lar risk score, baseline Mini-Mental State Examination
Remitter Status
scores, and baseline MADRS depression scores withthe 5 cognitive domain residualized change scores.
Some prior research suggests that cognitive
Fazekas scores were not normally distributed and
improvement over the course of treatment may vary
Am J Geriatr Psychiatry 20:8, August 2012
Copyright American Association for Geriatric Psychiatry. Unauthorized reproduction of this
TABLE 2. Correlations of Predictor Variables With Residualized Change Scores (Baseline to Posttreatment) in Each Cognitive Domain Variable Language Function Processing Speed Working Memory Episodic Memory Executive Function
− 0.18a
− 0.25c
− 0.17a
− 0.24c
− 0.24c
− 0.17a
− 0.16a
− 0.16a
− 0.19a Note: N = 166. Bold variables indicate siginificance and p>.05 or less. MMSE, Mini-Mental State Examination.
as a function of whether an individual was considered
older individuals with depression and to determine
to have remitted to treatment in terms of depression
whether factors such as the degree of vascular burden,
status.22,30 Thus, we examined cognitive change as a
white matter hyperintensities, and/or age of onset
function of remitter status, with a remitter defined as
influenced the degree to which cognition improved
someone who achieved a final MADRS score of 7 or
during treatment in late-life depression. We found
less. Of the 166 individuals with neuropsychological
that both episodic memory and executive function
data at both baseline and follow-up, 63 were remitters
improved from baseline to posttreatment and that this
and 103 were not. We computed a repeated-measures
improvement occurred for individuals whose depres-
analysis of variance with time (baseline, posttreat-
sion remitted and for those whose depression did
ment) and cognitive domain as within-subject factors
not remit. However, working memory improved only
and remitter status as a between-subject factor. This
among individuals with depression whose depres-
analysis of variance again revealed a time by cog-
sion remitted. Of note, we cannot definitely attribute
nitive domain interaction, F(4,656) = 9.92, p <0.001
these changes to the treatment, as we did not have
and revealed a main effect of remitter status, F(1,164)
a placebo control group. However, importantly, we
= 8.37, p = 0.004. However, there was no signifi-
found that a number of factors moderated the degree
cant two-way interaction between remitter status and
of improvement in cognition (whether it was specif-
time, F(1,164) = 1.24, p = 0.27, or three-way interaction
ically due to treatment or responsivity to practice)
between remitter status, time, and cognitive domain,
particularly among those individuals whose depres-
F(4,656) = 1.56, p = 0.184. As shown in Figure 2, the
sion did not fully remit. Specifically, older age, higher
main effect of remitter status reflected the fact that
vascular risk scores, and lower baseline Mini-Mental
the nonremitters had overall worse cognitive perfor-
State Examination scores predicted less improvement
mance than the remitters at both baseline and post-
in working memory. Furthermore, older age, later age
of onset, and higher vascular risk scores predictedless improvement in executive function. In addition,more severe white matter hyperintensities predicted
DISCUSSION
less improvement in processing speed.
The fact that episodic memory improved is consis-
The goal of the current study was to examine the
tent with prior work, suggesting that impairments
degree to which cognitive function improved dur-
in episodic memory may be associated with state
ing the course of antidepressant treatment among
components of depression and may be more likely
Am J Geriatr Psychiatry 20:8, August 2012
Copyright American Association for Geriatric Psychiatry. Unauthorized reproduction of this
Cognitive Change in Late-Life DepressionFIGURE 2. Graph of performance in each of the five cognitive domains at baseline and at posttreatment, plotted separately for those individuals whose depression remitted by the end of treatment (MADRS score ≤7) and for those individuals who depression did not remit by the end of treatment (see Supplemental Digital Content 1, http://links.lww.com/AJGP/A28).
to improve with the remission of depression than
sistent with the hypothesis that vascular changes lead-
some other cognitive functions.7 However, we also
ing to white matter alternations may contribute to
saw improvements in executive function, a domain
at least some of the cognitive impairments found in
in which improvements have not been as consistently
late-life depression.3–6 It is somewhat surprising that
demonstrated in prior studies.7 This is a cognitive
vascular burden and not white matter hyperinten-
domain that Douglas and Porter argued may reflect
sities predicted change in some of the other cogni-
more trait-like aspects of depression and which has
tive domains such as executive function and work-
been associated with white matter abnormalities in
ing memory. However, it may be that our measure of
late-life depression.3 Interestingly, the predictors of
white matter hyperintensities, which was restricted
change in episodic memory and executive function
to periventricular, deep white matter, and subcortical
were very different. The degree of change in execu-
gray matter regions, did not capture changes in white
tive function, but not episodic memory, was predicted
matter in other brain regions that may also be related
by older age, older age of onset, and higher vascular
risk scores. In contrast, baseline depression severity
We also found that individuals whose depression
predicted change in episodic memory but not exec-
remitted during treatment showed overall better cog-
utive function. Similar to executive function, change
nitive function. This result is consistent with our prior
in working memory was also predicted by older age
work (in this same sample) showing that baseline
and higher vascular risk scores. Thus, although both
cognitive function predicted response to treatment13
episodic memory and executive function improved
and with other work showing that impaired cogni-
over the course of treatment, the predictors of the
tive function in late-life depression is associated with
magnitude of change in executive function are con-
sistent with a critical role for vascular burden in
There were several limitations to this study. First,
constraining executive function (as well as working
we did not recruit a control sample of older adults
memory) and the degree to which it can improve in
without depression, as the purpose of the study
was to examine treatment response in older adults
In our prior work with this sample, we found that
with depression. Thus, we could not directly address
more severe white matter hyperintensities were asso-
the question of whether cognitive function in our
ciated with worse cognitive function in all domains
depressed individuals was worse than controls at
at baseline.13 Interestingly, in the current analyses,
baseline or whether the degree of cognitive improve-
we also found that more severe white matter hyper-
ment would have resulted in a level of cognitive
intensities predicted less improvement in processing
performance that no longer differed from individ-
speed. This relationship with processing speed is con-
uals without depression. However, the large body
Am J Geriatr Psychiatry 20:8, August 2012
Copyright American Association for Geriatric Psychiatry. Unauthorized reproduction of this
of research showing that late-life depression is asso-
ment that can be obtained in some domains among
ciated with impaired cognition relative to matched
older adults treated for depression. These results have
controls makes it likely that we would have also
important clinical implications in that they suggest
found that our sample was impaired relative to an
that a regular assessment of vascular risk in older
appropriate control group. Second, we did not have
adults with depression is necessary as a component
a placebo control group, so we cannot definitely
of treatment planning and in predicting prognosis,
determine that the cognitive change we did observe
both for the course of the depression itself and for the
reflected a response to treatment rather than prac-
cognitive impairments that often accompany depres-
tice effects or placebo effects. However, this does
not minimize the importance or utility of identify-ing predictors of cognitive change, regardless of the
The authors thank Dan Blazer M.D., Ph.D., for serv-
source of change. In other words, the ability to ben-
ing as an advisor to the study, Caroline Hellegers, M.A.,
efit from practice may be key to various cognitive
for her assistance with study coordination at Duke Univer-
enhancement approaches and thus information about
sity and Tony Durbin, M.S., and Brigitte Mittler for their
the factors that may identify who or who would
assistance with study coordination at Washington Univer-
show responsivity to either antidepressant therapy
sity. Drs. Sheline, Doraiswamy, and Taylor have received
or practice may be useful in individualized treatment
grants and/or speaking/consulting fees from antidepres-sant manufacturers but do not own stock in these compa-
In summary, we found that older adults with
nies. Dr. Krishnan is also a coinventor on a patent that is
depression showed significant improvement in
licensed to Cypress Biosciences and owns stock in CeneRx.
episodic memory and executive function across the
Dr. Doraiswamy also owns stock in EnergyInside.
course of a 12-week treatment with sertraline. Further-
This work was supported by a Collaborative R01 for
more, we found that factors such as age, age of onset,
Clinical Studies of Mental Disorders Grant MH60697
and vascular risk scores predicted the amount of
(YIS) and MH62158 (PMD). YIS also received support
change in cognitive domains such as executive func-
from NIMH K24 65421. In addition, this work was sup-
tion and working memory, a result consistent with the
ported by a grant (RR00036) to the WUSM General Clin-
hypothesis that vascular burden may play a critical
ical Research Center and by a grant from Pfizer, Inc., to
role in constraining the degree of cognitive improve-
References
1. Butters MA, Whyte EM, Nebes RD, et al: The nature and deter-
8. Baldwin RC, Gallagley A, Gourlay M, et al: Prognosis of late life
minants of neuropsychological functioning in late-life depression.
depression: a three-year cohort study of outcome and potential
Arch Gen Psychiatry 2004; 61(6):587–595
predictors. Int J Geriatr Psychiatry 2006; 21(1):57–63
2. Sheline YI, Barch DM, Garcia K, et al: Cognitive function in late life
9. Potter GG, Kittinger JD, Wagner HR, et al: Prefrontal neuropsycho-
depression: relationships to depression severity, cerebrovascular
logical predictors of treatment remission in late-life depression.
risk factors and processing speed. Biol Psychiatry 2006; 60(1):58–
Neuropsychopharmacology 2004; 29(12):2266–2271
10. Alexopoulos GS, Kiosses DN, Heo M, et al: Executive dysfunc-
3. Sheline YI, Price JL, Vaishnavi SN, et al: Regional white mat-
tion and the course of geriatric depression. Biol Psychiatry 2005;
ter hyperintensity burden in automated segmentation distin-
guishes late-life depressed subjects from comparison subjects
11. Sneed JR, Keilp JG, Brickman AM, et al: The specificity of neu-
matched for vascular risk factors. Am J Psychiatry 2008; 165(4):
ropsychological impairment in predicting antidepressant non-
response in the very old depressed. Int J Geriatr Psychiatry 2008;
4. Alexopoulos GS: Vascular disease, depression, and dementia. J Am
12. Story TJ, Potter GG, Attix DK, et al: Neurocognitive correlates of
5. Alexopoulos GS: The vascular depression hypothesis: 10 years
response to treatment in late-life depression. Am J Geriatr Psychi-
later. Biol Psychiatry 2006; 60(12):1304–1305
6. Barnes DE, Alexopoulos GS, Lopez OL, et al: Depressive symp-
13. Sheline YI, Pieper CF, Barch DM, et al: Support for the vascular
toms, vascular disease, and mild cognitive impairment: findings
depression hypothesis in late-life depression: results of a 2-site,
from the Cardiovascular Health Study. Arch Gen Psychiatry 2006;
prospective, antidepressant treatment trial. Arch Gen Psychiatry
7. Douglas KM, Porter RJ: Longitudinal assessment of neuropsycho-
14. Alexopoulos GS, Kiosses DN, Choi SJ, et al: Frontal white matter
logical function in major depression. Aust N Z J Psychiatry 2009;
microstructure and treatment response of late-life depression: a
preliminary study. Am J Psychiatry 2002; 159(11):1929–1932
Am J Geriatr Psychiatry 20:8, August 2012
Copyright American Association for Geriatric Psychiatry. Unauthorized reproduction of this
Cognitive Change in Late-Life Depression
15. Simpson SW, Baldwin RC, Burns A, et al: Regional cerebral vol-
27. Nebes RD, Butters MA, Mulsant BH, et al: Decreased working
ume measurements in late-life depression: relationship to clinical
memory and processing speed mediate cognitive impairment in
correlates, neuropsychological impairment and response to treat-
geriatric depression. Psychol Med 2000; 30(3):679–691
ment. Int J Geriatr Psychiatry 2001; 16(5):469–476
28. Bhalla RK, Butters MA, Mulsant BH, et al: Persistence of neuropsy-
16. O’Brien JT, Lloyd A, McKeith I, et al: A longitudinal study
chologic deficits in the remitted state of late-life depression. Am J
of hippocampal volume, cortisol levels, and cognition in
older depressed subjects. Am J Psychiatry 2004; 161(11):
29. Nakano Y, Baba H, Maeshima H, et al: Executive dysfunction in
medicated, remitted state of major depression. J Affect Disord
17. Castaneda AE, Tuulio-Henriksson A, Marttunen M, et al: A review
on cognitive impairments in depressive and anxiety disorders with
30. Culang ME, Sneed JR, Keilp JG, et al: Change in cognitive function-
a focus on young adults. J Affect Disord 2008; 106(1–2):1–27
ing following acute antidepressant treatment in late-life depres-
18. Grant MM, Thase ME, Sweeney JA: Cognitive disturbance in outpa-
sion. Am J Geriatr Psychiatry 2009; 17(10):881–888
tient depressed younger adults: evidence of modest impairment.
31. Zanardi R, Cusin C, Rossini D, et al: Comparison of response
to fluvoxamine in nondemented elderly compared to younger
19. Savaskan E, Muller SE, Bohringer A, et al: Antidepressive ther-
patients affected by major depression. J Clin Psychopharmacol
apy with escitalopram improves mood, cognitive symptoms, and
identity memory for angry faces in elderly depressed patients. Int
32. First MB, Spitzer RL, Gibbon M, et al: Structured clinical interview
J Neuropsychopharmacol 2008; 11(3):381–388
for the DSM-IV-TR Axis I disorders. Washington, DC, American
20. Gallassi R, Di Sarro R, Morreale A, et al: Memory impairment in
patients with late-onset major depression: the effect of antidepres-
33. Cipriani A, La Ferla T, Furukawa TA, et al: Sertraline versus other
sant therapy. J Affect Disord 2006; 91(2–3):243–250
antidepressive agents for depression. Cochrane Database Syst Rev
21. Doraiswamy PM, Krishnan KR, Oxman T, et al: Does antidepres-
sant therapy improve cognition in elderly depressed patients? J
34. DeVane CL, Pollock BG: Pharmacokinetic considerations of
Gerontol A Biol Sci Med Sci 2003; 58(12):M1137–M1144
antidepressant use in the elderly. J Clin Psychiatry 1999; 60(suppl
22. Devanand DP, Pelton GH, Marston K, et al: Sertraline treatment
of elderly patients with depression and cognitive impairment. Int
35. Montgomery SA, Asberg M: A new depression scale designed to
J Geriatr Psychiatry 2003; 18(2):123–130
be sensitive to changes. Br J Psychiatry 1979; 134:382–389
23. Butters MA, Becker JT, Nebes RD, et al: Changes in cognitive func-
36. Wolf PA, D’Agostino RB, Belanger AJ, et al: Probability of stroke: a
tioning following treatment of late-life depression. Am J Psychiatry
risk profile from the Framingham Study. Stroke 1991; 22:312–318
37. Jeerakathil T, Wolf PA, Beiser A, et al: Stroke risk profile pre-
24. Beats BC, Sahakian BJ, Levy R: Cognitive performance in tests sen-
dicts white matter hyperintensity volume: the Framingham Study.
sitive to frontal lobe dysfunction in the elderly depressed. Psychol
38. Seshadri S, Wolf PA, Beiser A, et al: Stroke risk profile, brain vol-
25. Abas MA, Sahakian BJ, Levy R. Neuropsychological deficits and
ume, and cognitive function: the Framingham Offspring Study.
CT scan changes in elderly depressives. Psychol Med 1990;
39. Morris JC: The Clinical Demential Rating (CDR): current version
26. Nebes RD, Pollock BG, Houck PR, et al: Persistence of cognitive
and scoring rules. Neurology 1993; 43:2412–2414
impairment in geriatric patients following antidepressant treat-
40. Folstein MF, Folstein SE, McHugh PR: Mini-Mental State: a practical
ment: a randomized, double-blind clinical trial with nortriptyline
method for grading the cognitive state of patients for the clinician.
and paroxetine. J Psychiatr Res 2003; 37(2):99–108
Am J Geriatr Psychiatry 20:8, August 2012
Copyright American Association for Geriatric Psychiatry. Unauthorized reproduction of this
DIABETES CONTROL MATTERS A CLOSER LOOK AT ORAL AGENTS FOR THE PATIENT Today, there are several kinds of oral agents, ordiabetes pills, available for the treatment of type 2diabetes. If you have type 2 diabetes, your doctorand health care team can help you decide which oralagent or combination of oral agents are the best foryou. Here are some general tips about oral agents:• Many doctor
Human Reproduction Update, Vol.7, No.1 pp. 70±77, 2001Sherman J.SilberInfertility Center of St Louis, St Luke's Hospital, 224 South Woods Mill Road, Suite 730, St Louis, MO 63017, USAThere is probably no subject that is more controversial in the area of male infertility than varicocele. Theoverwhelming majority of non-urologist infertility specialists in the world are extremely sceptical of th
 Cognitive Change in Late-Life Depression
TABLE 1. Demographic, Clinical, and Cognitive Characteristics of Participants
Cognitive Change in Late-Life Depression
TABLE 1. Demographic, Clinical, and Cognitive Characteristics of Participants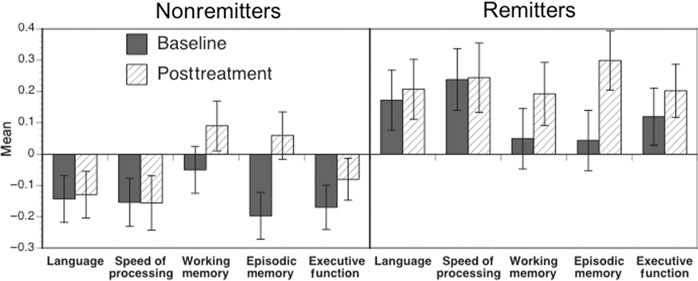 Cognitive Change in Late-Life Depression
FIGURE 2. Graph of performance in each of the five cognitive domains at baseline and at posttreatment, plotted separately for
Cognitive Change in Late-Life Depression
FIGURE 2. Graph of performance in each of the five cognitive domains at baseline and at posttreatment, plotted separately for