La spécificité du tadalafil est liée à sa longue demi-vie, permettant une action qui excède largement celle des autres inhibiteurs de PDE5. L’absorption digestive est complète, avec un pic plasmatique atteint en 2 heures environ. Le métabolisme est réalisé via CYP3A4, produisant des métabolites inactifs éliminés principalement dans les fèces. La sélectivité enzymatique est élevée, réduisant les effets indésirables extra-caverneux. Les réactions indésirables fréquentes incluent céphalées, bouffées vasomotrices et troubles digestifs légers. L’activité pharmacologique est stable, indépendamment de l’ingestion d’aliments. Dans les comparaisons de longue durée, acheter cialis pas cher est mentionné en relation avec les études portant sur la persistance d’efficacité et la constance de la cinétique plasmatique.
Hrup451 70.77
Human Reproduction Update, Vol.7, No.1 pp. 70±77, 2001
Sherman J.SilberInfertility Center of St Louis, St Luke's Hospital, 224 South Woods Mill Road, Suite 730, St Louis, MO 63017, USA
There is probably no subject that is more controversial in the area of male infertility than varicocele. The
overwhelming majority of non-urologist infertility specialists in the world are extremely sceptical of the role of
varicocele or varicocelectomy in the treatment of male infertility. Directors of most assisted reproductive
technologies (ART) programmes view the enthusiasm with which urologists approach varicocelectomy as a potential
impediment to the couple that is getting older and do not have much time left to become pregnant using ART. There
are many credible, well-controlled studies which show no effect of varicocelectomy on fertility. There are also a few
`controlled' studies that favour varicocelectomy, but all can be criticised on the basis of patient selection bias. Thus
the great weight of evidence from controlled studies is against varicocelectomy and the reports supporting
varicocelectomy are extremely weak. Finally, the reports that semen parameters are improved by varicocelectomy is
¯awed by uncontrolled observations and the failure to take into account the variability of semen analysis in infertile
men and its regression toward the mean. Many control studies have demonstrated that, because of this variability,
men with an initially low sperm count tend later to have higher sperm counts in the absence of any treatment
Key words: ART/pregnancy rate/semen parameters/varicocelectomy
sperm injection (ICSI) as an effective therapy for all cases of male
infertility which have failed to respond to conventional treatment
has caused a major reassessment and critical analysis of the
Lack of effect of varicocele on pregnancy rate following vasova-
diagnostic and therapeutic approaches to male infertility (Van
Steirteghem et al., 1993). In that light, the varicocelectomy
Controlled studies challenging the effectiveness of varicocelectomy
Controlled studies supporting varicocelectomy
Does varicocele cause a progressive decline in fertility?
In May 1998, an azoospermic patient of ours ®nally had twin boys
after a fourth cycle of testicular sperm extraction (TESE) and
ICSI. He had undergone bilateral varicocelectomy at a major
university 2 years earlier, for a sperm count of 19 Q 106
spermatozoa/ml, with a volume of 10 ml, and 60% sperm motility
There have been many years of debate over the causes and
with normal morphology, and had suffered complete left testicular
therapy of male infertility. Many treatments have been strongly
infarction and right testicular atrophy. His wife's pregnancy was
advocated for male infertility over the past four decades, e.g.
no thanks to her husband's varicocelectomy. A different patient
clomiphene citrate, testosterone, human menopausal gonadotro-
who had sperm counts that ¯uctuated between 2.8 and 94 Q 106
phin (HMG), human chorionic gonadotrophin (HCG), corticos-
spermatozoa/ml had a similar experience several years earlier,
teroids (for sperm antibodies), cold wet athletic supports,
and also required TESE±ICSI. These occasional complications of
vitamins, and even more recently very aggressively marketed
varicocelectomy have been known for >20 years (Silber, 1979).
nutritional supplements such as `Proxceed', without any docu-
Of course, this is not the usual disastrous result with bilateral
mented evidence of effectiveness (Devroey et al., 1998). It is
varicocelectomy. In fact, a microsurgical approach to varicoce-
becoming clear that many spermatogenic defects in the human are
lectomy has been designed to avoid such complications (Silber,
genetic in origin, and clearly impervious to improvement with any
1979; Goldstein et al., 1992; Marmar and Kim, 1994; Girardi and
current therapy (Reijo et al., 1995; Silber et al., 1995, 1998; Page
Goldstein, 1997; Scherr and Goldstein, 1999). Nonetheless, the
et al., 1999). Furthermore, the development of intracytoplasmic
occasional serious risk of varicocelectomy cannot be disregarded.
Ó European Society of Human Reproduction and Embryology
If it were not for this risk, microsurgical approaches to
out in the other 37 vasectomy reversal patients who had a
varicocelectomy would never have been developed. The more
varicocele. There was no statistically signi®cant difference
common risk of post-operative hydrocele (5%) is obviously just a
between the two groups (although their major point was the
nuisance and not as serious as devascularization (Dubin and
safety of performing simultaneous varicocelectomy).
Semen analyses are often highly variable, and spontaneous
pregnancies without treatment are so common that there is much
scepticism about many treatments for male infertility (Baker et
In 1995, Nieschlag proposed a basic axiom that needs to be
al., 1981, 1984, 1985, 1993; Baker and Kovacs, 1985; Baker and
followed in male infertility treatment: `Therapeutic interventions
Burger, 1986; Baker, 1986, 1993; Silber, 1989a; Devroey et al.,
in male infertility should be based on properly controlled clinical
1998; Devroey, 1999). Because no treatment of male infertility is
trials' (Nieschlag et al., 1995). Several reports on spontaneous
without risk, if for no other reason than simply the delaying of
pregnancy rates with no treatment in couples with severe male
more effective treatment until the wife is older, I would like to
factor justify Nieschlag's axiom. In 1993, Hargreave reported on
review in this paper the pitfalls of trying to evaluate either
patients with severe oligozoospermia, high serum FSH concen-
pregnancy results or sperm count results in patients undergoing
trations, and varicocele whose wives became pregnant after an
varicocelectomy or, indeed, any other treatment for male
initial infertility consultation without any treatment of the male
infertility, without properly controlled studies.
(Hargreave and Elton, 1983; Hargreave, 1993). A total of 33% of
men in this category had a varicocele, and did not have time to
Lack of effect of varicocele on pregnancy rate following
undergo varicocelectomy before their wife became pregnant. The
point of his study was that, with alarmingly low sperm counts,
women can become pregnant without any treatment of the male,
In 1989, we reported a 10 year follow-up of men undergoing
verifying concepts that have been clear for many years (Smith et
vasovasostomy (who had spermatozoa in the vas ¯uid without
al., 1977; Zukerman et al., 1977; Steinberger and Rodriguez-
secondary epididymal blowouts), and their long-term results
(Silber, 1989b). This experience was the origin of my scepticism
To understand the importance of a controlled study in
regarding the value of varicocelectomy. Out of 282 patients
evaluating the validity of varicocelectomy, one has only to look
undergoing vasovasostomy ten or more years earlier, who had
at the spontaneous conception rates in the wives of men with
good sperm in the vas ¯uid (meaning there was no secondary
various low sperm counts. Hargreave and Elton's work was not
epididymal obstruction), 42 (14.8%) had a discernible (moderate
just about varicocelectomy, but also was about the issue of `what
or large) varicocele upon physical examination, and 240 (85.2%)
is male infertility' (Hargreave and Elton, 1983; Silber, 1989a).
had no such varicocele (Table I). These men had no other medical
They found that even in men with sperm counts of `2 Q106
or surgical treatment other than vasovasostomy. The wives of
spermatozoa/ml, and with a duration of infertility of as long as 4
78.5% of those men with varicocele (not operated upon), became
years, 20% of the wives eventually have a spontaneous
pregnant, and the wives of 81.2% of those without varicocele
conception without ever having any improvement in the sperm
became pregnant. Thus, there was no statistically signi®cant
count. In men with sperm counts of 5 Q 106 spermatozoa/ml with
difference (78.5 versus 81.2%) in pregnancy rate in those with
only 1 year of infertility, 36% of the wives became pregnant
varicocele versus those without varicocele for older men under-
without any treatment (Table II). Thus, if one had performed a
going vasovasostomy. There was also no difference in post-
varicocelectomy on such men prior to their wife's conception,
operative semen parameters. Our conclusion from this study was
without a controlled study, we might have mistakenly concluded
that in a group of men with prior fertility who have a varicocele
that the operation is what enabled the pregnancy, even though it
(who were fertile except for their vasectomy, but many years later
was simply a spurious, unrelated event.
decide to have their vasectomy reversed) the presence of a
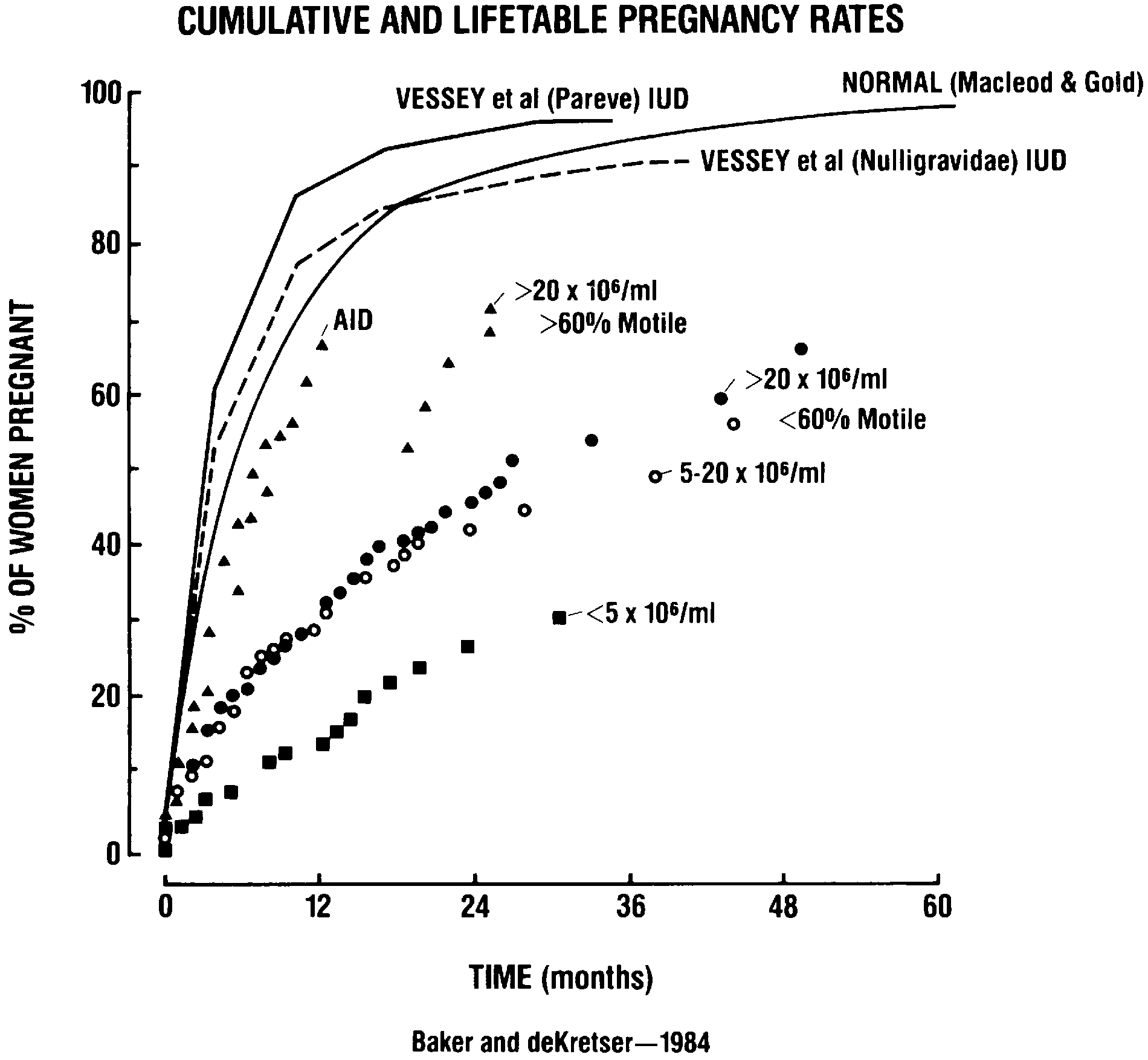
Baker and Burger in 1986, reported life-table pregnancy rates
varicocele did not have any discernible effect on their long-term
over 3 years in couples with varying categories of semen
parameters compared to control groups (Baker and Burger, 1986).
A decade later, essentially the same question was addressed
Although lower sperm counts resulted in lower pregnancy rates, a
(Mulhall et al., 1997) when varicocelectomy was performed
simultaneously with vasovasostomy in 10 vasectomy reversal
patients who had varicocele but varicocelectomy was not carried
Table II. Percentage chance of conception for the next year (wife with normal
results after investigation) (Hargreave and Elton, 1983)
Table I. Lack of effect of varicocoele (not operated on) on pregnancy rate
following vasovasostomy (taken from Silber, 1989b). Values in parentheses
substantial percentage of couples achieved pregnancy sponta-
couples would not have become pregnant without the surgery.
neously despite severe oligoasthenozoospermia (Figure 1).
Nieschlag concluded in 1998, as did Mordel in 1990, `Studies
In 1983, Schoysman reported an extensive 12 year experience
since 1952 advocating varicocelectomy have been uncontrolled
following 1291 oligozoospermic men who underwent no
and not evidence-based' (Mordel et al., 1990; Nieschlag et al.,
improvement in semen parameters (Schoysman and Gerris,
1983). They found that for men with sperm counts of 1±5 Q
It is easy to become enthusiastic about any treatment of male
106 spermatozoa/ml, 12% of wives became pregnant within 5
infertility that is performed without adequate controls. In a series
years and 27% of wives became pregnant within 12 years without
of men with either azoospermia or extremely severe oligozoos-
any treatment (Table III). Even when the sperm count was <1
permia, the pregnancy rate in 56 severely oligozoospermic men
Q106 spermatozoa/ml, 4% of wives conceived spontaneously
following varicocelectomy was 23% (13 out of 56), and for
within 5 years, and 9% within 12 years without any treatment.
`azoospermic' men was 9% (two out of 22) (Steckel et al., 1993;
When sperm counts were 15±20 Q 106 spermatozoa/ml, 69% of
Matthews et al., 1998). The problem with these studies again is
wives became pregnant within 5 years and 82% within 12 years,
that there is no control group, no longitudinal follow-up, and it
again with no treatment of the male. These studies demonstrate
pays no attention to the concept of `regression toward the mean.'
the dif®culty of interpreting whether any treatment of the male
More recently a similar study (Kim et al., 1999) resulted in no
with oligozoospermia, e.g. varicocelectomy, has any discernible
spontaneous pregnancies even in the varicocelectomy group even
though these authors maintained that sperm count `improved'
In 1975, Amelar and Dubin compiled a summary of all
after surgery. Once again there is no control group of similar
varicocelectomy studies prior to that time (Dubin and Amelar,
patients who did not receive surgery. We all have seen men who
1975). None of the 11 papers on varicocelectomy published by
are initially azoospermic, who will eventually, in subsequent
1975 was controlled. Most of them showed ~60±70% of patients
semen analyses, have spermatozoa in the ejaculate without any
had an improvement in sperm count, and most of the studies
treatment (MacLeod and Gold, 1953; Baker and Kovacs, 1985).
showed pregnancy rates from a low of 30% to a high of 55%.
Without a control group to compare with, one should not be
None of the studies controlled for the pregnancy rate in couples
surprised to see a spontaneous pregnancy rate of 9±23% without
not undergoing varicocelectomy, and just assumed that these
any treatment of the male partner with severe sperm defects,
particularly if the couple has had a short period of infertility, and/
or if the wife is young (Hargreave and Elton, 1983; Schoysman
Varicocelectomy and sperm countMacLeod and Gold, as far back as 1951 (MacLeod and Gold,
1951; MacLeod and Gold, 1953), ®rst demonstrated that sperm
concentration and motility tend to increase with time with
repeated testing in oligozoospermic and asthenozoospermic men
despite no treatment. This was a peculiar mathematical quirk
related to the highly variable nature of the sperm count. That
means that, without any treatment whatsoever, if you continue to
get sperm counts and semen analyses longitudinally on men who
initially have low sperm counts and poor motility, the low sperm
count and the poor motility will routinely tend to increase with
repeated tests and no treatment (MacLeod and Gold, 1951, 1953).
Baker et al. were the ®rst to clearly and mathematically explain
this phenomenon of `regression toward the mean' (Baker et al.,
1981; Baker and Kovacs, 1985; Baker, 1986). `Regression toward
Figure 1. Cumulative and life-table pregnancy rates (Baker and Burger, 1986).
the mean' has profound implications for all clinical trials.
Whenever there is a highly variable measurement, if patients
have a controlled period followed by a treatment period, there is
Table III. Pregnancy rates in 1291 oligozoospermic men (Schoysman and
likely to be a signi®cant improvement even if the treatment is
ineffective. Baker et al. observed the same phenomenon that
McLeod and Gold had observed 30 years earlier, that sperm
concentration and motility increased progressively in their study
of day-to-day variability of semen analyses in infertile men.
Sperm motility increased equally on both active drug and on
placebo treatment in a double-blind controlled trial of erythro-
mycin for asthenozoospermia (Baker et al., 1984). Clearly,
erythromycin had no impact whatsoever on either sperm count or
sperm motility. However, in this double blind control study, it was
obvious that the sperm motility increased in an equal manner in
patients that were on erythromycin and patients that were on
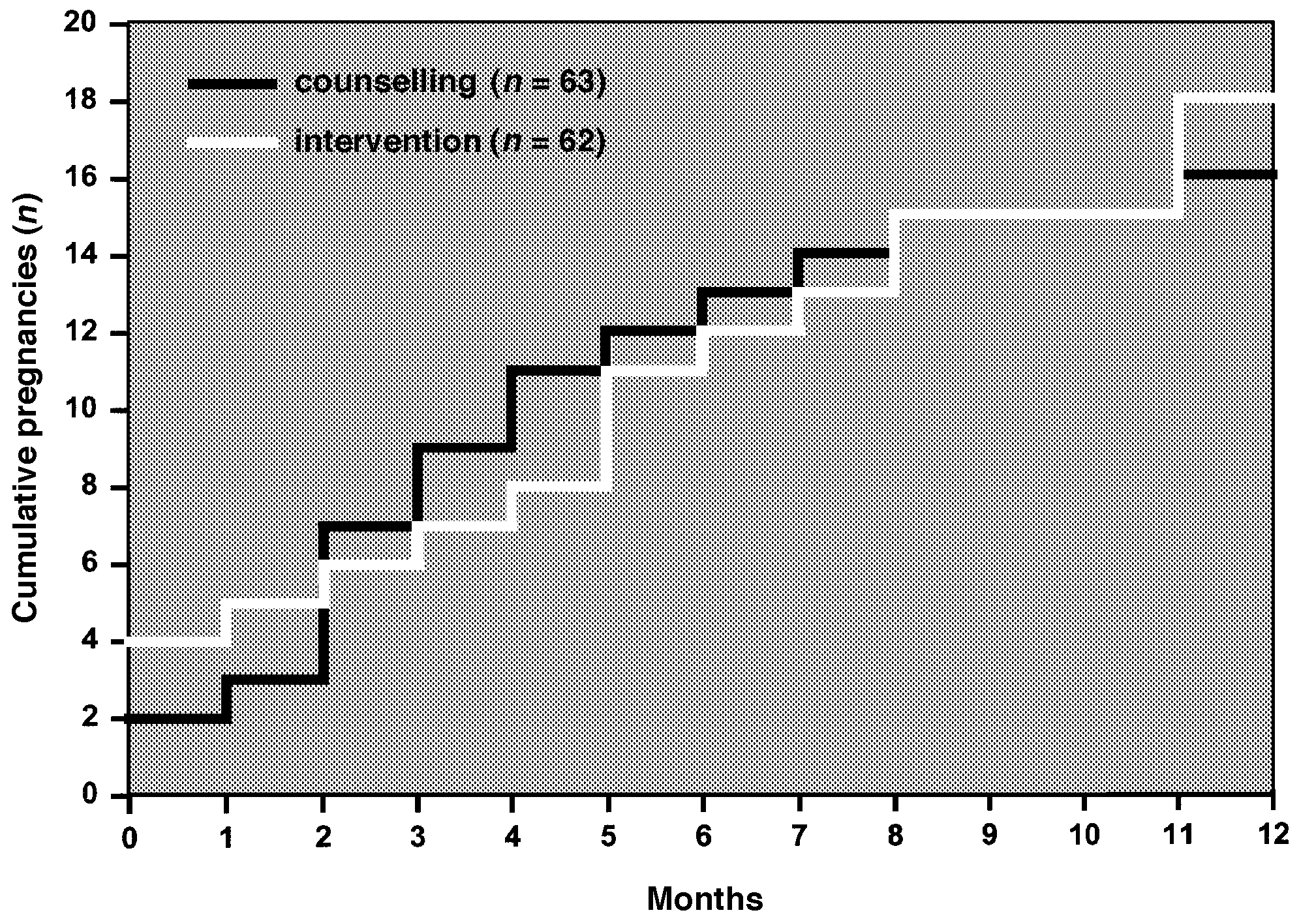
63 of them underwent counselling. It is important to point out that
placebo. `In a similar fashion, sperm motility increased in men
it was not just a `treatment versus no treatment' group, but rather
with varicoceles whether or not they had testicular vein ligations
it was a `surgical varicocelectomy treatment group' versus a
performed' (Baker et al., 1985). No matter what the treatment,
`psychological counselling group' (Figure 2) shows the survival
whether erythromycin, or watchful waiting, clomiphene citrate or
curve results of the two different groups. There was no signi®cant
varicocelectomy, an initially low sperm count (because of
difference in pregnancy rate measured over time between those
intrinsic variability) will gravitate higher because of `regression
couples that underwent varicocelectomy and those couples that
underwent psychological counselling. Furthermore, Nieschlag's
Baker and Kovacs also concluded in 1985 that `a group of
group found no relationship of pregnancy to semen parameters,
subjects selected for low results will on average have higher
hormone concentrations, grade of varicocele, or the age of the
results on re-measurement' (Baker and Kovacs, 1985). This
male. The only relationship to pregnancy rate was the age of the
phenomenon of `regression toward the mean' signi®es that
wife and that was the only factor that could help predict the
whenever you have a phenomenon that is highly variable, and
you have a select group of couples on the low end of that
Nieschlag's controlled study attempted to put us on a more
phenomenon, whether sperm count or sperm motility, because of
scienti®c footing in evaluating varicocelectomy, and also helped
the intrinsic variability, repeated tests will generally show an
us realize how differences in the population characteristics of the
increase which has nothing to do with biology but is simply a
wives of these infertile men would have potentially a major
mathematical event that has to occur. As Baker and Kovacs
confounding effect. For example, one might, without proper
showed, therefore, a low sperm count will generally improve,
control studies, be very enthusiastic about varicocelectomy in a
with or without any treatment. Similarly, a very high sperm count
practice involving younger couples, and less enthusiastic in a
will generally become worse with or without any treatment. Men
practice involving older ones. We discovered a similar confound-
with an average ®rst sperm count of 28 Q 106 had an average
ing phenomenon in the treatment of obstructive azoospermia with
second sperm count of 56 Q 106. Men with an average ®rst sperm
count of 271 Q 106 had a mean second sperm count of 145 Q 106.
Table IV. Obstructive azoospermia and intracytoplasmic sperm injection
Among 216 semen donors whose initial motility averaged 42%,
(ICSI): female age-related variation in pregnancy rate
the second semen analysis showed a mean of 55% motility. Thus,
whenever uncontrolled varicocelectomy studies mention an
improvement in motility, or sperm count, this is what one often
would expect to ®nd with no treatment whatsoever when you are
beginning with oligozoospermic couples (Baker and Kovacs,
Controlled studies challenging the effectiveness of
varicocelectomyNieschlag's group performed a very meticulously controlled study
to attempt to evaluate the effect of varicocelectomy (Nieschlag et
al., 1995, 1998). They studied 125 infertile couples with
varicocele. Of those couples, 62 underwent varicocelectomy and
Figure 3. Life-table curves of pregnancy rates for before ligation (n) and after
ligation (s) groups. Number of patients initially and those followed up to the
end of each year is shown at top of ®gure. Symbols indicate those months in
which the life table changed, i.e. pregnancies occurred. Although some
patients were followed up for >5 years (those in before ligation group for
Figure 2. Cumulative pregnancy rates over 12 months in couples with male
maximum of 92 months, after ligation group for 108 months), the longest
varicocele treated by intervention (ligation or embolization) or counselling
duration of follow up to pregnancy was 60 months. There was no signi®cant
alone (taken from Nieschlag et al., 1998. Previously published in Hum.
difference between the two curves by log rank test (Baker et al., 1985.
Reprinted with permission from British Medical Journal).
sperm retrieval and ICSI. The only factor that signi®cantly
spermatozoa/ml. Of patients with sperm counts of >10 Q 106
affected the variation in pregnancy rate in couples undergoing
spermatozoa/ml, those who conceived had a mean sperm count of
ICSI with retrieved spermatozoa was the age of the wife (Silber et
40 Q 106 spermatozoa/ml, and those who did not conceive had a
al., 1997) (Table IV). The delivery rate with ICSI using retrieved
mean sperm count of 48 Q 106 spermatozoa/ml.
spermatozoa was 44% in women under aged <30 years; 34% with
In 1979, Nilsson et al. questioned the ef®cacy of varicoce-
women aged 30±36; 13% with women ages 37±39; and only 4%
lectomy with a boldly titled paper: `Improvement of semen and
with women aged >40 years the delivery rate per cycle. With
pregnancy rate after ligation and division of the internal spermatic
women aged <37 years, who also had a good ovarian reserve, the
vein: Fact or ®ction?' (Nilsson et al., 1979). They randomized
delivery rate was 42%. Thus, it seems that in any kind of
their patients to 51 having varicocelectomy and 45 serving as
infertility treatment for male factor, regardless of sperm count,
controls. All had similar varicocele characteristics and all the
and whether for varicocele or obstructive azoospermia, the most
patients had suffered 2±8 years of infertility. Varicocelectomy
important confounding factor, aside from duration of infertility, is
produced no change in semen parameters. Most importantly,
the age and ovarian reserve of the wife.
pregnancies were achieved in four out of 51 (8%) patients
In the controlled varicocele study performed earlier by Baker's
undergoing varicocelectomy, and in eight out of 45 (17%) having
group (Baker et al., 1985), 651 infertile couples with varicocele
were studied for pregnancy rate per month with or without
In 1992, Rageth et al. studied 89 patients with varicocele, poor
varicocelectomy. Biases due to any difference in prognostic
semen, and duration of infertility of up to 7 years (Rageth et al.,
factors were allowed for by using the Cox regression analysis. Of
1992). Of the 56 patients undergoing varicocelectomy, the wives
the couples, 324 had sperm counts of <20 Q 106 spermatozoa/ml
of 23 (41%) became pregnant eventually with treatment. Of the
and 327 had sperm counts of >20 Q 106 spermatozoa/ml. There
33 who did not undergo varicocelectomy, the wives of 14 became
was no signi®cant difference in the sperm concentration or
pregnant (42%) with treatment. Thus, there was no difference at
motility after varicocelectomy. There was no difference in
all in pregnancy rate between those who had surgery and those
pregnancy rate after varicocelectomy. Figure 3 demonstrates the
who did not. Rageth et al. observed an improvement in sperm
pregnancy rate of these couples over a course of 5 years. Looking
count after surgery from 9 to 15 Q 106 spermatozoa/ml, an
at the `before ligation' and the `after ligation' groups reveals that
improvement in morphology from 22 to 28%, and an improve-
the two curves essentially overlap each other. There is no
signi®cant difference in log rank test between these curves. In
In all fairness, we need to mention the peculiarities of some of
fact, in the ®rst few months of the study, the pregnancy rate
these control studies in the following critical way. In the study of
appeared to be higher before varicocele ligation but eventually
Baker et al. (1985), the sperm count did not improve with
after 1 or 1/2 years, the curves had completely coalesced (Baker et
varicocelectomy, but sperm motility improved equally with or
without varicocelectomy. Patients who had a varicocele did have
The studies of Nieschlag's group in 1995 and 1998, and the
a higher pregnancy rate than those who did not have a varicocele
study by Baker et al. a decade earlier, seemed to dampen any
whether operated on or not. In Rodriguez-Rigau et al.'s group, the
overwhelming enthusiasm for varicocelectomy on the part of
sperm count and motility improved after varicocelectomy, but
many infertility physicians, even though there is still registered
pregnancy rate was not affected (Rodriguez-Rigau et al., 1978). In
throughout the urology world a strong defensive posture regarding
Nieschlag et al.'s group, the sperm count increased in the
this procedure. There were, however, other controlled studies, not
varicocelectomy group, but not in the control group. Sperm
quite as carefully designed as the aforementioned, that also
motility did not change with or without varicocelectomy. Sperm
revealed the shaky ground on which the pro-varicocelectomy
morphology decreased simply over time in both groups, the
forces stood. In 1986, Vermuelen from Belgium reported on 90
patients undergoing varicocelectomy and 25 patients not under-
Additional criticisms have been offered on the Nieschlag study.
going varicocelectomy. Both groups were comparable in terms of
It does not appear to be well-controlled for varicocele size, and
duration of infertility, age, sperm count, and motility. Cumulative
the follow-up was limited only to several years. In Vermeulen's
pregnancy rates in these two groups were the same over a 12
study (1986), some patients in the non-operated group got
month follow-up period. Interestingly, both groups showed
pregnant before surgery could be performed. In Nilsson's group
`slightly improved sperm characteristics' (Vermeulen et al.,
(1979), the pregnancy rates were rather low in both groups,
though they may not be a valid criticism since they were treating
In 1978, Rodriguez-Rigau et al. from Texas reported a large
couples with a long duration of infertility in an older age group.
group of patients which was not prospective and not randomized,
Despite these possible criticisms, for the most part the control
but was controlled, some of whom underwent varicocelectomy
studies showing no effect of varicocelectomy have been viewed
and others who did not (Rodriguez-Rigau et al., 1978).
by most andrologists to be reliable.
Rodriguez-Rigau et al. noted a slightly increased percentage
motility in patients undergoing varicocelectomy. However, there
Controlled studies supporting varicocelectomy
was no difference in pregnancy rate among those who had
varicocelectomy versus those who did not. Furthermore, there was
There have been three reported `control' studies that suggest a
no relation of improvement in post-operative sperm count to
bene®cial effect of varicocelectomy. Marmar and Kim (1994),
pregnancy rate. Those patients who conceived after varicocelect-
reviewed retrospectively a series of 466 varicocelectomies and
omy had a mean sperm count of 28 Q 106 spermatozoa/ml and
only 19 controls. Of the 466 couples that underwent
those who did not conceive had a mean sperm count of 26 Q 106
varicocelectomy, 186 became pregnant (pregnancy rate
35.6%). The pregnancy rate in the small number of 19
the question of whether or not varicocele really created `stress'
`controls' that did not undergo varicocelectomy was 15.8%.
that results eventually in deterioration of testicular function.
The large difference in the size of the varicocelectomy group
As far back as 1968, Uehling studied the fertility of 440
and the control group certainly suggests an unwitting selection
married men in the military coming in for routine physical
bias. This kind of a skewed population would make it very
examination, with and without varicoceles. Of this group, 138 had
likely that the `controls' were simply people whose semen was
no children (31.4%) and 302 did have children (68.6%). To break
so poor that there was no desire to undergo surgery, or
it down further, of the 75 men with a varicocele, 69% had
possibly there may have been a problem with the wife that
children and of the 227 men without a varicocele, 68% had
made surgery also very problematic. At any rate, being a
children. Thus, there was no difference in fatherhood of those
retrospective study with such unbalanced varicocelectomy
young married military recruits who had varicocele versus those
control groups, indicates a probable selection bias.
who did not have varicocele. The presence or absence of a
Another `control' study often referred to is that of Girardi and
varicocele in these young men had no in¯uence on whether or not
Goldstein in which 1500 infertile males underwent varicocelect-
their wives were able to get pregnant (Uehling, 1968). At least in
omy, and only 47 controls underwent varicocelectomy (Girardi
young men, varicocele seemed to have no negative impact on
and Goldstein, 1997). This is clearly the same problem of balance
between patients undergoing varicocelectomy and patients
So what is the prevalence of varicocele in a group of otherwise
serving as `controls' that occurred in the study of Marmar and
healthy young men? Thomason et al. in a similar study of military
Kim. They reported a 43% pregnancy rate in couples in whom the
recruits, in 1979, concluded, `It is apparent that the prevalence of
husband had a varicocelectomy and a 17% pregnancy rate in those
varicoceles in young men occurs with signi®cant frequency and
whose husbands did not have a varicocelectomy. They also noted
does not interfere with the fertility in all individuals' (Thomason
an improvement in sperm count from 40 to 47 Q 106
and Farris, 1979). It was found that 30.7% of all recruits had a left
spermatozoa/ml. This is not a very dramatic increase in mean
varicocele (14% were small, and 16.7% were moderate or large),
sperm count and is most likely simply related to `regression
and 29.4% of recruits who had fathered children also had a
toward the mean.' This study also suffers from a great likelihood
varicocele (15% were moderate or large). This is similar to the
of selection bias in that only 3% of the men in the study were
frequency of large or moderate left varicocele in older vasectomy
`controls' for the other 97% who had surgery.
reversal patients (Silber, 1989b). They concluded, `the prevalence
The World Health Organization (WHO) study was an attempt
of a left-sided varicocele occurs with such frequency among a
to settle the varicocele issue employing thousands of couples in a
group of healthy men that one would question the association of a
multi-centre trial design (WHO, 1992). This study was never
varicocele and poor semen quality.' Although I have observed no
published in its original form because of problems with protocol
difference in fertility after vasovasostomy in older men with or
deviations (Nieschlag et al., 1995, 1998). It is very dif®cult with
without varicocele, there are, nonetheless, many other reports
multi-centre studies involving a highly controversial subject to be
which suggest a deterioration caused by varicocele as one gets
certain that all programmes that want to serve their patients in the
way they think is best, can stick to a rigid protocol. However,
It has been commonly thought that secondary infertility, (i.e.
such a rigid protocol would be necessary in order to give the study
the couple gets pregnant without treatment for their ®rst child, and
credibility (WHO, 1992). One group that pulled out of the WHO
then cannot get pregnant years later when they want another one)
study did publish the results of 45 couples out of their 210 who
was due to increased age and declining fertility of the female
were split off from the original group of 9034 infertile couples
(Nieschlag et al., 1995, 1998; Silber et al., 1997). Gorelick and
originally entering the study, 1326 of whom had a clinical
Goldstein, however, have suggested that a varicocele is found in
varicocele. This group maintained that varicocelectomy did have
35% of men with primary infertility, and in 81% of men with
a bene®cial effect. However, such a splitting off from the original
secondary infertility, implying that secondary infertility is caused
study group of ®ve times as many patients as originally started,
by declining semen parameters related to the long-term
even in their local programme and representing only 3% of the
deleterious effect of an uncorrected varicocele (Gorelick and
original WHO couples, has a great risk of unwitting selection bias
Goldstein, 1993). Out of 1001 men with `primary' infertility, 352
(35%) had a varicocele on routine physical examination, but when
couples came for `secondary' infertility,' 79 out of 98 (81%) had
Does varicocele cause a progressive decline in fertility?
a varicocele present. This is an impressive incidence of ®nding a
varicocele in infertile couples. Witt and Lipshultz (1993) have
For years, urologists talked about an excess number of `tapered'
made a similar claim that 50% of couples with primary infertility
forms of spermatozoa, i.e. the `stress pattern,' as a distinctive
have a varicocele and 69% of couples with secondary infertility
feature of patients with varicocele. It was called a `stress pattern'
have a varicocele (Witt and Lipshultz, 1993).
to re¯ect what was thought to be a `stress' on testicular function
The authors suggested this meant that over time the presence of
created by the varicocele. However, Baker et al. in 1985
a varicocele causes a diminution in sperm quality and indeed is
questioned whether there is a `speci®c abnormality of sperm
the major cause of secondary infertility. This would suggest a
morphology with varicoceles?' In fact, they found no signi®cant
need for varicocelectomy in virtually all young men with a
difference in the morphological patterns with or without
varicocele in order to prevent subsequent decline of testicular
varicocele. Contrary to popular myth, there was `no characteristic
function. That's a lot of varicocelectomies. Of course, there were
morphologic stress pattern in infertile men with large left
some problems with these reports. Firstly, there was no
varicoceles' (Baker et al., 1981, 1985; Baker, 198). This raised
demonstrated decline in sperm count caused by the varicocele,
but rather simply an increased incidence of varicocele found in
varicocele in adolescents with reduced left testicular size may
the older couples. Secondly, the mean FSH concentration in their
have a long-term effect on sperm count, if not on fertility, requires
patients with primary infertility was 7.9 IU/ml, and in their
a carefully controlled longitudinal study. In science, our minds
patients with secondary infertility the mean FSH was 17.6 IU/ml.
must always remain open, and not be driven by what we merely
These ®ndings are confusing in that one would not expect an FSH
to be so elevated in men with mean sperm counts of 30 Q 106
spermatozoa/ml. Thirdly, the group of men de®ned as having
primary male infertility had normal mean sperm counts.
Nonetheless, if other centres were able to con®rm that 81% of
older couples with secondary infertility have a varicocele, and
Baker, G. (1992) The use of the semen analysis in predicting fertility outcome.
only 20% of younger couples with primary infertility have a
[Editorial comment.] Aust. N.Z. J. Obstet. Gynecol., 32, 154±155.
Baker, H.W.G. (1986) Requirements for controlled therapeutic trials in male
varicocele, the conclusion would be enormous in terms of
infertility. Clin. Reprod. Fertil., 4, 13±25.
recommending varicocelectomy for 15±35% of the entire world.
Baker, H.W.G. (1993) Management of immunological infertility. In Berger,
On the contrary however, other authors have demonstrated no
H.G. and Oshima, H. (eds), An Approach to Clinical Andrology. Serona
difference in the incidence of varicocele in men with primary or
Symposia Reviews, no. 29, pp. 105±110.
Baker, H.W.G. and Burger, H.G. (1986) Male infertility in reproductive
secondary infertility (Jarow et al., 1996). They found the primary
medicine. In Steinberger, E., Frajese, G., Steinberger, A. (eds.)
determinant of secondary infertility was the age of the wife. We
Reproductive Medicine. Raven Press, New York, USA, pp. 187±197.
have also found no such increase in the incidence of varicocele
Baker, H.W.G. and Kovacs, G.T. (1985) Spontaneous improvement in semen
quality: regression towards the mean. Int. J. Androl., 8, 421±426.
either in secondary infertility or in other men with infertility. So
Baker, H.W.G., Burger, H.G., de Kretser, D.M. et al. (1981) Factors affecting
this fascinating speculation that in 81% of couples with secondary
the variability of semen analysis results in infertile men. Int. J. Androl., 4,
infertility, the cause is varicocele, may not turn out to be valid.
Infertility centres see many older couples who did not try to
Baker, H.W.G., Straffon, W.G.E., McGowan, M.P. et al. (1984) A controlled
trial of the use of erythromycin for men with asthenospermia. Int. J.
have their baby when they were in their 20s. These couples might
very well have been couples with `secondary' infertility if it were
Baker, H.W.G., Burger, H.G., de Kretser, D.M. et al. (1985) Testicular vein
not for the fact that they did not marry until they were 35 and did
ligation and fertility in men with varicoceles. Br. Med. J., 291, 1678±
not already have children. One would expect in this group of older
Baker, H.W.G., Liu, D.Y., Bourne, H. and Lopata, A. (1993) Diagnosis of
couples also to see a higher incidence of varicocele if the presence
sperm defects in selecting patients for assisted fertilization. Hum. Reprod.,
of varicocele over the period of time causes a decline in fertility
and/or sperm count. However, we do not see a higher incidence of
Devroey, P., Vandervorst, M., Nagy, P. and Van Steirteghem, A. (1998) Do
varicocele in older couples than in younger couples coming in for
we treat the male or his gamete? Hum. Reprod., 13 (Suppl 1), 178±185.
Devroey, P. (1999) The relevance of semen analysis. Presented at Thirty-
primary infertility. Furthermore, we have found no difference in
Second Annual Postgraduate Program of the American Society for
pregnancy rate or semen parameters with long-term follow-up of
Reproductive Medicine in Toronto, Canada, September 1999. pp. 15±32.
older vasovasostomy patients who did or did not have a varicocele
Dubin, L. and Amelar, R.D. (1975) Varicocelectomy as therapy in male
Girardi, S.K. and Goldstein, M. (1997) Varicocele. Curr. Ther. Endocrinol.
However, there are studies which suggest that varicocelectomy
may be of bene®t in some selected cases. In 1991, Wensing's
Goldstein, M., Gilbert, B.R., Dicker, A.P. et al. (1992) Microsurgical inguinal
group in Holland studied testis volumes, semen quality and
varicocoelectomy with delivery on the testis: an artery and lymphatic
morphological patterns of spermatozoa in adolescents with and
sparing technique. J. Urol., 148, 1808±1811.
Gorelick, J.I. and Goldstein, M. (1993) Loss of fertility in men with
without varicocele, trying to nail down the issue of whether early
varicocele. Fertil. Steril., 59, 613±616.
varicocelectomy could be recommended as a preventative in
Haans, L.C.F., Laven, J.S.E., Mali, W.P.Th. M. et al. (1991) Testis volumes,
adolescents with left testicular atrophy (Haans et al., 1991; Laven
semen quality, and hormonal patterns in adolescents with and without
et al., 1992). They showed a small increase in the adolescent's left
varicocele. Fertil. Steril., 56, 731±736.
Hargreave, T.B. and Elton, R.A. (1983) Is conventional sperm analysis of any
testicular volume after varicocelectomy. They found that
`varicocele-related' unilateral or bilateral growth failure is not
Hargreave, T.B. (1993) Varicocele ± a clinical enigma. Br. J. Urol., 72, 401±
clearly associated with a decrease in sperm counts or semen
quality, but could be prevented by adolescent varicocelectomy in
Jarow, J.P., Coburn, M. and Sigman, M. (1996) Incidence of varicocoeles in
men with primary and secondary infertility. Urology, 47, 73±76.
those young men presenting with a left varicocele and a smaller
Kim, E.D., Leibman, B., Grinblat, D. and Lipshultz, L. (1999) Varicocele
left testicle. It was not clear, however, whether this `growth
repair improves semen parameters in azoospermeric men. J. Urol., 162
failure' continued during adulthood and could lead to future
disturbances in infertility. Differences in semen parameters were
Laven, J.S.E., Haans, L.C.F., Mali, W.P.T.M. et al. (1992) Effects of
varicocele treatment in adolescents: a randomized study. Fertil. Steril., 58,
not at all convincing. Furthermore, despite their enthusiasm for
studying the early impact of varicocele on testicular atrophy, they
MacLeod, J. and Gold, R.Z. (1951) The male factor in fertility and infertility.
could ®nd no evidence to suggest further deterioration of
II. Spermatozoon counts in 1000 men of known fertility and in 1000 cases
of infertile marriage. J. Urol., 66, 436±449.
MacLeod, J. and Gold, R.Z. (1953) The male factor in fertility and infertility.
I do not wish to conclude on a 100% negative note regarding
VI. Semen quality and other factors in relation to ease of conception.
the varicocele issue, because we must always have an open mind
in science. It appears fairly conclusive that varicocelectomy does
Madjar, I., Weissenberg, R., Lunenfeld, B. et al. (1995) Controlled trial of
high spermatic vein ligation for varicocele in infertile men. Fertil. Steril.,
not do much, if anything, to help the average infertile couple. That
should not be controversial. The speculation that the occasional
Marmar, J.L. and Kim, Y. (1994) Subinguinal microsurgical varicocelectomy:
A technical critique and statistical analysis of semen and pregnancy data.
Silber, S.J. (1989b) Pregnancy after vasovasostomy for vasectomy reversal: a
study of factors affecting long-term return of fertility n 282 patients
Matthews, G.J., Matthews, E.D. and Goldstein, M. (1998) Induction of
followed for 10 years. Hum. Reprod., 4, 318±322.
spermatogenesis and achievement of pregnancy after microsurgical
Silber, S.J., Nagy, Z., Liu, J. et al. (1995) The use of epididymal and testicular
spermatozoa for intracytoplasmic sperm injection: the genetic
oligoasthenospermia. Fertil. Steril., 70, 71±75.
implications for male infertility. Hum. Reprod., 10, 2031±2043.
Mordel, N., Mor-Yosef, S., Margalioth, E.J. et al. (1990) Spermatic vein
Silber, S.J., Nagy, Z., Devroey, P. et al. (1997) The effect of female age and
ligation as treatment for male infertility. J. Reprod. Med., 35, 123±127.
ovarian reserve on pregnancy rate in male infertility: treatment of
Mulhall, J.P., Stokes, S., Andrawis, R. and Buch, J.P. (1997) Simultaneous
azoospermia with sperm retrieval and intracytoplasmic sperm injection.
microsurgical vasal reconstruction and varicocele ligation: Safety pro®le
and outcomes. Urology, 50, 438±442.
Silber, S.J., Alagappan, R., Brown, L.G. and Page, D.C. (1998) Y chromosome
Nieschlag, E., Hertle, L., Fischedick, A. and Behre, H.M. (1995) Treatment of
deletions in azoospermic and severely oligozoospermic men undergoing
varicocele: counselling as effective as occlusion of the vena spermatica.
intracytoplasmic sperm injection after testicular sperm extraction. Hum.
Nieschlag, E., Hertle, L., Fischedick, A. et al. (1998) Update on treatment of
Smith, K.D., Rodriguez-Rigau, L.J. and Steinberger, E. (1977) Relation
varicocele: counselling as effective as occlusion of the vena spermatica,
between indices of semen analysis and pregnancy rate in infertile couples.
Nilsson, S., Edvinsson, A. and Nilsson, B. (1979) Improvement of semen and
pregnancy rate after ligation and division of the internal spermatic vein:
Steckel, J., Dicker, A.P. and Goldstein, M. (1993) Relationship between
Fact or ®ction? Br. J. Urol., 51, 591±596.
varicocele size and response to varicocelectomy. J. Urol., 149, 769±771.
Page DC, Silber S, Brown LG. (1999) Men with infertility caused by AZFc
Steinberger, E. and Rodriguez-Rigau, L.J. (1983) The infertile couple.
deletion can produce sons by intracytoplasmic sperm injection, but are
likely to transmit the deletion and infertility. Hum. Reprod., 14, 1722±
Thomason, M. and Farris, B.L. (1979) The prevalence of varicocele in a group
of healthy young men. Milit. Med., 144, 181±186.
Rageth, J.C., Unger, C., DaRugna, D. et al. (1992) Long-term results of
Uehling, D.T. (1968) Fertility in men with varicocele. Int. J. Fertil., 13, 58±60.
varicocelectomy. Urol. Int., 48, 327±331.
Van Steirteghem, A.C., Nagy, Z., Joris, H. et al. (1993) High fertilization and
Reijo, R., Lee, T., Salo, P. et al. (1995) Diverse spermatogenic defects in
implantation rates after intracytoplasmic sperm injection. Hum. Reprod.,
humans caused by Y chromosome deletions encompassing a novel RNA-
binding protein gene. Nature Genet., 10, 383±393.
Vermeulen, A., Vandeweghe, M. and Deslypere, J.P. (1986) Prognosis of
Rodriguez-Rigau, L.J., Smith, K.D. and Steinberger, E. (1978) Relationship of
subfertility in men with corrected or uncorrected varicocele. J. Androl., 7,
varicocele to sperm output and fertility of male partners in infertile
Witt, M. and Lipshultz, L. (1993) Varicocele: A progressive or static lesion?
Scherr, D. and Goldstein, M. (1999) Comparison of bilateral versus unilateral
varicocelectomy in men with palpable bilateral varicoceles. J. Urol., 162,
World Health Organization (1992) The in¯uence of varicocele on parameters
of fertility in a large group of men presenting to infertility clinics. Fertil.
Schoysman, R.G. and Gerris, J. (1983) Twelve-year follow-up study of
pregnancy rates in 1291 couples with idiopathically impathically impaired
Zukerman, Z., Rodriguez-Rigau, L.J., Smith, K.D. and Steinberger, E. (1977)
male fertility. Acta Eur. Fertil., 14, 51±56.
Frequency distribution of sperm counts in fertile and infertile males.
Silber, S.J. (1979) Microsurgical aspects of varicocele. Fertil. Steril., 31, 230±
Silber, S.J. (1989a) The relationship of abnormal semen parameters to male
Received on February 3, 2000; accepted on November 8, 2000
fertility. [Opinion.] Hum. Reprod., 4, 947±953.
James C. Wittig, MD Orthopedic Oncologist Percutaneous Radiofrequency Ablation (RFA) The latest, “State of the Art Treatment” for Osteoid Osteoma is PERCUTANEOUS RADIOFREQUENCY ABLATION (also known as RFA). This is a minimally invasive procedure that is performed under a CAT Scan, usually by a highly specialized musculoskeletal radiologist, in which a needle or probe is in
 substantial percentage of couples achieved pregnancy sponta-
couples would not have become pregnant without the surgery.
substantial percentage of couples achieved pregnancy sponta-
couples would not have become pregnant without the surgery.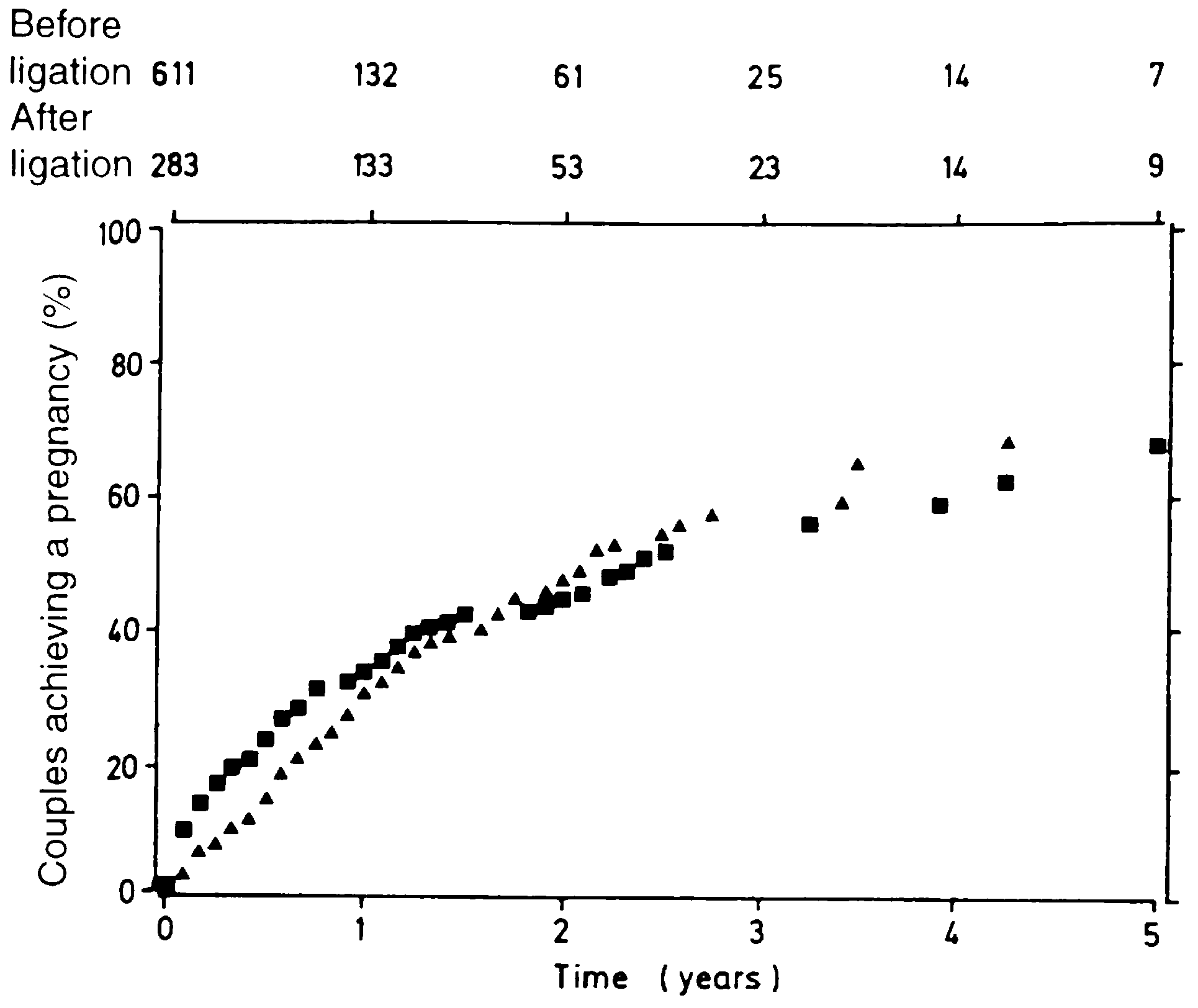
 patients that were on erythromycin and patients that were on
63 of them underwent counselling. It is important to point out that
placebo. `In a similar fashion, sperm motility increased in men
it was not just a `treatment versus no treatment' group, but rather
with varicoceles whether or not they had testicular vein ligations
it was a `surgical varicocelectomy treatment group' versus a
performed' (Baker et al., 1985). No matter what the treatment,
`psychological counselling group' (Figure 2) shows the survival
whether erythromycin, or watchful waiting, clomiphene citrate or
curve results of the two different groups. There was no signi®cant
varicocelectomy, an initially low sperm count (because of
difference in pregnancy rate measured over time between those
intrinsic variability) will gravitate higher because of `regression
couples that underwent varicocelectomy and those couples that
underwent psychological counselling. Furthermore, Nieschlag's
Baker and Kovacs also concluded in 1985 that `a group of
group found no relationship of pregnancy to semen parameters,
subjects selected for low results will on average have higher
hormone concentrations, grade of varicocele, or the age of the
results on re-measurement' (Baker and Kovacs, 1985). This
male. The only relationship to pregnancy rate was the age of the
phenomenon of `regression toward the mean' signi®es that
wife and that was the only factor that could help predict the
whenever you have a phenomenon that is highly variable, and
you have a select group of couples on the low end of that
Nieschlag's controlled study attempted to put us on a more
phenomenon, whether sperm count or sperm motility, because of
scienti®c footing in evaluating varicocelectomy, and also helped
the intrinsic variability, repeated tests will generally show an
us realize how differences in the population characteristics of the
increase which has nothing to do with biology but is simply a
wives of these infertile men would have potentially a major
mathematical event that has to occur. As Baker and Kovacs
confounding effect. For example, one might, without proper
showed, therefore, a low sperm count will generally improve,
control studies, be very enthusiastic about varicocelectomy in a
with or without any treatment. Similarly, a very high sperm count
practice involving younger couples, and less enthusiastic in a
will generally become worse with or without any treatment. Men
practice involving older ones. We discovered a similar confound-
with an average ®rst sperm count of 28 Q 106 had an average
ing phenomenon in the treatment of obstructive azoospermia with
second sperm count of 56 Q 106. Men with an average ®rst sperm
count of 271 Q 106 had a mean second sperm count of 145 Q 106.
patients that were on erythromycin and patients that were on
63 of them underwent counselling. It is important to point out that
placebo. `In a similar fashion, sperm motility increased in men
it was not just a `treatment versus no treatment' group, but rather
with varicoceles whether or not they had testicular vein ligations
it was a `surgical varicocelectomy treatment group' versus a
performed' (Baker et al., 1985). No matter what the treatment,
`psychological counselling group' (Figure 2) shows the survival
whether erythromycin, or watchful waiting, clomiphene citrate or
curve results of the two different groups. There was no signi®cant
varicocelectomy, an initially low sperm count (because of
difference in pregnancy rate measured over time between those
intrinsic variability) will gravitate higher because of `regression
couples that underwent varicocelectomy and those couples that
underwent psychological counselling. Furthermore, Nieschlag's
Baker and Kovacs also concluded in 1985 that `a group of
group found no relationship of pregnancy to semen parameters,
subjects selected for low results will on average have higher
hormone concentrations, grade of varicocele, or the age of the
results on re-measurement' (Baker and Kovacs, 1985). This
male. The only relationship to pregnancy rate was the age of the
phenomenon of `regression toward the mean' signi®es that
wife and that was the only factor that could help predict the
whenever you have a phenomenon that is highly variable, and
you have a select group of couples on the low end of that
Nieschlag's controlled study attempted to put us on a more
phenomenon, whether sperm count or sperm motility, because of
scienti®c footing in evaluating varicocelectomy, and also helped
the intrinsic variability, repeated tests will generally show an
us realize how differences in the population characteristics of the
increase which has nothing to do with biology but is simply a
wives of these infertile men would have potentially a major
mathematical event that has to occur. As Baker and Kovacs
confounding effect. For example, one might, without proper
showed, therefore, a low sperm count will generally improve,
control studies, be very enthusiastic about varicocelectomy in a
with or without any treatment. Similarly, a very high sperm count
practice involving younger couples, and less enthusiastic in a
will generally become worse with or without any treatment. Men
practice involving older ones. We discovered a similar confound-
with an average ®rst sperm count of 28 Q 106 had an average
ing phenomenon in the treatment of obstructive azoospermia with
second sperm count of 56 Q 106. Men with an average ®rst sperm
count of 271 Q 106 had a mean second sperm count of 145 Q 106.