La spécificité du tadalafil est liée à sa longue demi-vie, permettant une action qui excède largement celle des autres inhibiteurs de PDE5. L’absorption digestive est complète, avec un pic plasmatique atteint en 2 heures environ. Le métabolisme est réalisé via CYP3A4, produisant des métabolites inactifs éliminés principalement dans les fèces. La sélectivité enzymatique est élevée, réduisant les effets indésirables extra-caverneux. Les réactions indésirables fréquentes incluent céphalées, bouffées vasomotrices et troubles digestifs légers. L’activité pharmacologique est stable, indépendamment de l’ingestion d’aliments. Dans les comparaisons de longue durée, acheter cialis pas cher est mentionné en relation avec les études portant sur la persistance d’efficacité et la constance de la cinétique plasmatique.
Course:
Chapter 21
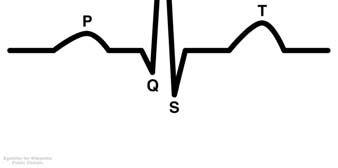
Cardiovascular conduction Best seen with an ECG. Cardiac muscle cells are kind of like loaded springs – a small electrical impulse sets them off and they depolarize and contract. Repolarization is the equivalent of setting up the spring again.
☯ P Wave on the left is an indicator of the depolarization of the
SA (sino-atrial) node which contracts both the left and the right atria.
☯ The span from the P to the R indicates the electical impulses
passing from the SA node to the AV (atrioventricular) node.
☯ The QRS segment, often called the QRS complex,
corresponds to the depolarization (contraction) of the left and right ventricles. The impulses are traveling from the AV node through the Bundle of His (pronounced “hiss”) and the Purkinje fibers at this point. Ventricular contractions are much more forceful than the atrial contractions which is why it spikes like this. The atria are repolarizing (getting ready for the next contraction) while this is going on.
☯ The T wave represents the repolarization of the ventricals.
At depolarization the sodium ions are entering the cell. During repolarization the potassium ions are leaving the cell. The autonomic nervous system and the heart The heart is autorhythmic and initiates it’s own beat. The autonomic nervous system however regulates the heart rate and force of contraction.
Releases norepinephrine to increase heart rate and force of contraction.
Releases ACH to decrease the heart rate and force of contraction.
Disease of the heart Congestive heart failure (CHF)
Characterized by poor contractile ability to pump, so it pumps less blood than it receives. Blood then accumulates in the chambers of the heart causing dilation and enlargement of the organ. This results in less blood circulating in the vessels.
Low blood flow in the Kidneys triggers the Kidneys to retain more water and electrolytes leading to fluid retention and edema. More water/fluid retention in the body creates a lot of hydraulic pressure also resulting in hypertension.
Fluid goes to lungs and interferes with gas exchange causing shortness of breath.
Fluid goes to the abdomen causing ascites and lower extremity edema.
Failure on one side leads to failure on the other side. Treated with:
Cardiac glycosides, diuretics, vasodilators. More on that shortly.
Coronary Artery Disease (CAD)
This is insufficiency of blood flow through the coronary arteries. Any abnormal reduction in coronary blood flow means a lowered functional ability of the heart.
Happens with aging, hardening and narrowing of the arteries leading to lowered blood flow.
Narrowing and hardening of the arteries due to fatty deposits on the arterial walls. Same result: lowered blood flow.
Chest pain due to insufficient blood flow in the coronary arteries. Can be related to arterio-, atherosclerosis and coronary artery spasms. Usually happens with physical exertion or psychological stress, but can occur for other reasons too. Treated with vasodilators and antianginals.
Heart attack. If the myocardium is deprived of blood or there is low blood flow for a long time (ischemia) then the tissues of the heart die or necrose. A complete blockage or thrombosis of a coronary artery is an MI. A large MI is sudden death. A smaller MI kills heart muscle cells which is replaced by non-functional scar tissue on the heart which reduces the available contractile tissue of the heart and thus the heart function. Can result in CHF and arrhythmias of the heart.
Chapter 22
Cardiac glycosides General These come from Digitalis purpurea and D. lanata. Therapetuic doses of glycosides:
1. Increase force of myocardial muscle contraction in CHF in which there is a higher need for
2. Decreases the heart rate and directly depresses the AV node conduction in the heart wall because
You can see this at the S-T segment of an ECG as well as in the T wave. You’ll also see a loner PR wave indicating slower AV node conduction. If the dose of glycosides is too high, however it lowers the AV conduction to the point where it blocks the heart. If a patient’s pulse is not 60-100 bpm or if the patient is arrhythmic, don’t use glycosides! Mechanisms of action for glycosides
☯ Calcium ions enter the heart muscle causing an increased force of contraction. ☯ ATP is inhibited so that more sodium accumulates in the cells. Sodium exits the cardiac
muscle cells at depolarization/contraction, so more sodium = stronger contraction.
All of this means the heart has a stroner contraction in a shorter time which increases blood circulation thus lowering heart blood congestion.
Pharmacokinetics of glycosides
Digitalization is the loading dose of cardiac glycoside which gets the process above going. Once the patient is “digitalized” you drop back to a lower maintenance dose to maintain the serum level of the drug in the body. Food will delay the timing of the absorption of glycosides, but not the amount absorbed.
Clinical indications
Atrial fibrillation, CHF, atrial tachycardia, and to lower the ventricular contraction rate.
Serum electrolyte levels and cardiac glycosides
Glycosides are affected by electrolyte levels, especially potassium and calcium. Since diuretics are often added to cardiac glycosides in drug therapy and these can totally jack with the levels of potassium, sodium and calcium all of these fun interactions are possible:
Decreased potassium levels. Sensitizes heart to toxic effects of glycosides causing increased arrhythmias, ventricular fibrillation and death.
Increased potassium levels antagonize the effects of glycosides
Increased serum calcium levels which enhances the actions of glycosides and can cause arrhythmias.
Adverse and toxic effects
Adverse effects are usually due to overdose. Include N/V, HA, visual disturbances, rashes. The fix is to lower the dose. Toxic effects are serious and include arrhythmias. Usually in the form of ectopic (extra) beats, premature ventricular contractions. Can also cause ventricular tachycardia, ventricular defibrillation, and cardiac arrest. The fix is to stop glycosides, increase calcium and give antiarrhythmics. For serious glycoside intoxication use digibind an antidigoxin antibody to bind the drug so it is no longer for pharmaceutical functions.
There are two. They’re both “-oxin” drugs. Both have a low therapeutic index and adverse/toxic effects above therapeutic levels.
☯ Digoxin
Not significantly bound to plasma proteins. Excreted through urine mostly unmetabolized. ½ life is 1.5 – 2 days, longer in the elderly.
☯ Digitoxin
More lipid soluble than digoxin and requires more metabolizing by the liver. Excreted through the urinary and GI tract. ½ life is 5 – 7 days.
Drug interactions
These lower the absorption of glycosides in the GI tract:
☯ Antacids ☯ Laxatives ☯ Kaolinpectin ☯ Cholestyramine
Decreases heart rate and force of contraction
☯ Verapamil ☯ Diltiazen ☯ Beta blockers
Diuretics such as thiazides and organic acids decrease potassium levels causing hypokalemia and glycoside toxicity.
Diuretic therapy and CHF Used to eliminate excess sodium and water via urinary excretion. Can be used alone or with glycosides (hence the warnings about serum electrolyte levels above). The result is a lowering of excess blood volume and blood congestion meaning the heart functions better. More on diuretics in a bit. Vasodilator therapy and CHF Relaxes and dilates the blood vessels (both veins and arteries) lowering peripheral resistance and blood pressure. This lowers the cardiac demand and oxygen consumption. Drugs that dilate the arteries/arterioles are better for lowering blood pressure and also decrease venous blood return to the heart, further reducing heart demands. More on this as well later on. Other therapies for CHF include
ACE inhibitors (chapter 26 material) and are preferred to vasodilators because they have less toxic effects and risks than vasodilators + glycosides.
Chapter 23
Arrhythmias are common with CHF, CAD, MI, and chronic drug therapy. They can cause palpitations to cardiac arrest. The severity of them determines their funciton on heart function and blood pressure. Types of arrhythmias Generally these occur when the electrical impulses in the heart are impaired. They cause premature contractions, tachycardia, flutter and fibrillation. The heart functions because of the interaction of sodium, potassium and calcium. An arrhythmia is a disturbance of the movement of these ions and the properties of the heart. Antiarrhythmic drugs affect the electrophysical properties of the heart membrane and these ions. Type of arrhythmia
These originate at the atria and AV node
Areas of abnormal impulse generation. Can occur when the electical impulses are delayed or blocked.
Electrical impulses are very disturbed and ventricles cannot maintain circulation of blood.
Class 1 antiarrhythmic drugs These all possess local anesthetic properties. They interfere with the sodium ions at the depolarization phase, in the heart membranes and excitable tisues. They also slow the conduction velocity, prolong the refractory period and therefore decrease the automaticity of the heart. Quinidine
Comes from the bark of the chinchona tree.
Treats: Supraventricular arrhythmias such as atrial flugger and fibrilation as well as various ventricular arrhythmias. Pharmacological effects: This is a cardiac depressant and decreases myocardial conduction
☯ Decreases force of contraction at higher doses. ☯ Lowers excitability of action potential tissues of the heart ☯ Slows conduction of electrical impulses through heart tissues thus supression the ectopic
foci and other electrical disturbances associated with arrhythmias.
Pharmacokinetics: Absorbs well in the GI tract, excreted thru the urine. Metabolizes to active metabolites so if the liver is not functioning well can lead to toxic buildup. Toxic levels produce arrhythmias (ironic, no?), CHF, and possible cardiac arrest. Adverse effects:
☯ Commonly seen: N/V/D and irritation of the GI tract. ☯ Chinchonism syndrome:
o Tinnitus, dizziness, salivation, HA, hallucinations
☯ Hypotension ☯ Weakness, fatigue, dyspnea ☯ Rare side effects:
o Hepatitis, thrombocytopenia with bleeding problems
☯ Hyperkalemia and excess potassium supplementation increases quinidine toxicity. Since
potassium is a cardiac depressant can depress heart and cause arrhythmias.
☯ Contraindicated with patients with AV block esp due to digitalis toxicity. Results in
☯ Increases Digitalis plasma levels, so digitalis must be reduced when used with quinidine. ☯ Inhibits other drugs’ metabolisms, especially beta blockers like propranolol.
Procainamide (Procanbid)
Synthetic, related to procaine (a local anesthetic). Pharmacological effects: Same as quinidine. This is a cardiac depressant and decreases myocardial conduction. This drug has a shorter ½ life than quinidine – 12 hour doses given.
☯ Fewer at a therapeutic dose than quinidine, but still N/V, anorexia, skin rash ☯ Chronic use: SLE type butterfly rash and arthralgia ☯ Widens PR, QRS, and Q-T waves so can increase appearance of premature bveats. ☯ Hi doses: cardiac depression ☯ Rare: agranulocytes leading to increased risk of infection.
Disopyramide (Norpace)
☯ Cardiac depression, slowing conduction rate and force ☯ Lowers heart excitability ☯ Supresses ectopic foci and other arrhythmias due to slower conduction impulses. ☯ Prolongs refractory period
Treats atrial and ventricular arrhythmias. Side effects:
☯ Dry mouth ☯ Visual disturbances ☯ Constipation ☯ Urinary retention ☯ Higher doses:
o Depression of heart o CHF with predisposition to heart failure
Lidocaine (Xylocaine)
Synthetic, often used for a local anesthetic, but also for ventricular arrhythmias (especially ectopic foci). Most often used for MI or during surgery as it does not depress normal impulse conduction, but does depress automaticity. Has to be IV or IM due to short acting time Adverse effects:
☯ Rapid metabolism at liver so if liver is damaged the levels will be higher ☯ At high concentration can cause convulsions since it is a CNS stimulant ☯ At toxic concentration will anesthesize CNS leading to cardiac and respiratory arrest.
Mexiletine (Mexotil) and Tocainide (Tonocard)
Derivatives of lidocaine, used orally. Same effects as lidocaine, used to treat ventricular arrhythmias for outpatients.
Phenytoin (Dilantin)
Originally used as an anti-epileptic, used in cardio to treat ventricular arrhythmias esp d/t digitalis and AV block. Phenytoin increases AV conduction and possibly eliminates AV block. Side effects:
☯ Common: blurry vision, vertigo, nystagmus (involuntary eye movements) ☯ Higher doses: hyperglycemia, so danger for diabetics, renal failure/insufficiency. ☯ Chronic use: gingival hyperplasia!
Other Class 1’s are newer and are used when other antiarrhythmics fail: Flecainide, Moricizine, Propafenone.
Class 2 antiarrhythmic drugs Beta-adrenergic blockers. In heart disease there is an increase in sympathetic activity and in norepinephrine/epinephrine. There is therefore an increase in heart rate, excitability, conduction velocity, and automaticity, especially in the ventricles. There is also a reduced refractory period. All of these lead to arrhythmias. You can reduce all of the above by blocking norepinephrine/epinephrine. Propranolol (Inderal)
Widely used and quinidine like in function. Depresses cardiac membranes at higher doses. Used to treat supraventricular and ventricular arrhythmias. Can be combined with Class 1 drugs for control of arrhythmias.
☯ Slows heart rate ☯ Reduces AV conduction ☯ Prolongs refractory period
☯ Hypotension and bradycardia ☯ Skin rashes, confusion, visual disturbances ☯ Overdose:
Esmolol (Brevibloc)
Beta 1 receptor blocker in heart muscle. Given via IV as it has a short duration because of rapid metabolism. Adverse effects:
☯ Hypotension and bradycardia ☯ Delayed AV conduction
Class 3 antiarrhythmic drugs These interfere with efflux of potassium ions during the first thru third repolarization phases. This prolongs the refractory period and lessens the frequency of arrhythmias. Bretylium (Bretylol)
Adrenergic neuronal blocker which decreases the release of norepinephrine thus proloning refractory time at the ventricles. Treats resistant ventricular tachycardia/fibrillation. Due to poor GI absorption is given IM/IV. Adverse effects:
Amiodarone (Cordanone)
Potent. Used when others don’t work. Has a local anesthetic effect. Blocks pharmaceutical receptors for alpha, beta and calcium. Treats by prolonging the refractory period. Has a ½ life of about 60 days!
☯ Thyroid dysfunction: contains iodine. ☯ Causes corneal deposits and visual disturbances ☯ Skin discoloration and dermatitis ☯ Pulmonary fibrosis ☯ Liver dysfunction
Sotalol (Betapace)
Nonselective beta blocker. Prolongs refractory period, slows AV conduction, and decreases automaticity of the heart. Adverse effects similar to other beta blockers.
Class 4 antiarrhythmic drugs These are calcium antagonists and calcium channel blockers, reducing the ability of calcium to enter the cells which have electrophysical properties or cells with excitable membranes that develop action potentials. That’s a long way to say: heart and blood vessels. These drugs have 2 major functions.
1. Decrease the rate of SA node and thus the heart rate and the conduction velocity of the AV node.
They treat fast ventricular tachycardia, also called tachyarrhythmias.
2. By antagonizing calcium, they cause cardiac and smooth muscle to relax and vessels to dilate.
This reduces the force of contraction, treating angina pectoris and hypertension. The down side is this can lead the CHF if there’s too much of that noise.
Verapamil (Calan)
☯ Reduces SA node activity causing slight decrease in rate of heart contraction ☯ Reduces AV node conduction treating various AV node arrhythmias and other
☯ Is a vasodilator so treats angina pectoris.
HA, dizziness, minor GI disturbances such as constipation
☯ Hypotension, especially with a change in position (i.e., orthostatic hypotension) ☯ Cardiac depression leading to CHF and various degrees of heart blockage. Especially true
when used with other cardiac depressants
existing SA/AV node disturbances or with CHF
Diltiazem (Cardizem)
Less potent than verapamil as an antiarrhythmic but more potent as a vasodilator. Main use is antihypertensive (see chapter 26)
Other antiarrhythmics
Adenosine (Adenocard)
Commonly used in emergency situations and in IV for supraventricular tachycardia. You might recognize this one as a component of the ATP (adenosine triphosphate) cycle. When used in arrhythmic crisis will lower the AV node conduction, decrease SA node pacemaker activity to terminate supraventricular tachycardia. Has a very short duration time: 15 – 30 seconds. Adverse effects:
☯ Asystole ☯ Dyspnea ☯ Occasionally, bronchospasms
Chapter 24
Angina pectoris is pain in the chest. When coronary arteries are affected by arteriosclerosis and by atherosclerosis they cannot deliver enough oxygen to the heart during exertion so a condition of ischemia occurs. This is most often the cause of angina. If it happens at rest rather than during exertion it indicates a smasm of the smooth vessel walls, but still a decrease in blood flow and myocardial ischemia. This is a form of CAD (coronary artery disease) and is most often treated most effectively by diet of lower fat and cholesterol, exercise, cessation of smoking and weight control. Nitrates/Nitrites These sublingual drugs relieve angina pain when the body converts the nitrates/nitrites into nitrous oxide which relaxes the vascular smooth muscle to allow more blood flow in the body and creates less demand on the heart. At lower doses they have a great effect on the venous system. These drugs lower venous return (preload) and blood pressure (preload). Clinical use:
Used for acute anginal attacks. Begin to work in 1-3 minutes, best at 5 minutes.
Applied to chest or abdomen and covered with plastic dressing. Absorbs thru skin within 15 minutes, lasts up to 8 hours.
☯ Cutaneous flushing, dizziness, headaches, weakness, fainting. ☯ Tolerance develops over time, so dosage increase needed. Unfortunately, high doses will
oxidizes hemoglobin to methemoglobin which won’t carry oxygen. Leads to hypoxia and anemia.
☯ Contraindicated for glaucoma patients
Beta adrenergic blockers Reverses the effects of the sympathetic nervous system caused by exercise, physical/mental simulus. Reduces the heart rate/force and thus decreases the work load and oxygen consumption of the heart. This prevents the ischemia/pain. Used for long term management of angina. Most often used drug: Propranolol. Calcium antagonists Interferes with calcium goin thru the cell membranes. Contraction of vascular smooth muscle needs it – it’s used at membrane depolarization in the smooth muscle. When calcium is antagonized there is less vascular tone and the vessels dilate. This decreases venous return (preload) and blood pressure. Adverse effects for all Calcium blockers:
☯ Headache ☯ Face flushing ☯ Dizziness ☯ Hypotension ☯ Minor GI disturbances
Verapamil (Calan, Isoptin)
Does this feel like a déjà vu? It is. See chapter 23. Used for supravenricular arrhythmias and also vasodilates to treat angina. Lowers the heart rate/force. Adverse fx:
☯ Too large a dose will depress cardiac function. Can lead to CHF, bradycardia. ☯ Constipation
Diltiazem (Cardizem)
Been here and done this one too. Has fewer side fx than verapamil. Causes slight decrease in heart rate, but will vasodilate coronary arteries and causes a modest fall in BP. Adverse fx:
☯ Slows heart rate and can cause cardiac depression leading to CHF, bradycardia.
Nifedipine (Procardia)
Potent vasodilator, lowers BP. Minor effect on heart rate/contraction Adverse fx:
☯ Can cause reflex tachycardia if BP goes too low.
Nicardipine (Cardene)
Similar to Nifedipine. Main function is vasodilation and relaxation of coronary artery spasms. Adverse fx:
☯ Can cause reflex tachycardia if BP goes too low.
All but bepridil below will slow the heart rate and lower the force. They are all potent vasodilators and lower BP.
☯ Amlodipine (Norvasc) ☯ Bepridil – slows the rate and is an antiarrhythmic also ☯ Felodipine ☯ Isradipine
Chapter 25
The kidney maintains water and electolyte balance and therefore acid-base balance in the body. The kidney gets 25% of the cardiac output to perform this function well. The body needs both ions and water to function. The kidneys absorb essential elements from wastes and pass the rest along as urine. Nephrons are the functional units of the kidney. They consist of the glomerulus, PCT (primary convoluted tubule), the loop of Henle, DCT (distal convoluted tubule), and the collecting duct. Urine is produced in the nephrons via filtration, reabsorption and secretion. Filtration:
Substances are pulled out of the blood in the glomerulus.
Ions are pulled out of the nephron and back into the blood and this is called tubular reabsorption. Occurs in the PCT, loop, and DCT. Most important is sodium which goes back into circulation. 99% of sodium is reabsorbed here. Sodium ions are positively charged cations in the extracelllar fluids. They create an osmotic gradient to attract water molecules, so water balance is dependent upon sodium.
Tubular secretion occurs in the PCT, loop, and DCT. Substances are secreted which help ions, acids, and bases reabsorb. This is all about hydrogen ions and acid/base balance. Blood pH has to be between 7.34 and 7.42. One way to do this is to adjust what is absorbed and what is passed to the urine, changing the acid balance of urine as well (which ranges from pH 4 – 6). Another way is thru the production of bicarbonate. Carbonic anyhdrase produces hydrogen ions and bicarbonate ions from carbon dioxide and water. The bicarbonate can then be released back to the blood to neutralize cell wastes like lactic acid.
Any process interfering with this process then inteferes with the pH balance of the body. One example is acidosis, a result of insufficient bicarbonate production due to carbonic anhydrase inhibition. More on that soon. Normal cell metabolism produces uric acid, as well as other weak acids and bases. The PCT secretes weak acids/bases to the urine. A lot of drugs are also weak acids or bases and also secrete through the PCT to the urine. Metabolic waste products must then compete for the same realestate to get out of the body as the drugs do. This can result in altered drug excretion and accumulations of drugs or metabolic wastes in the body.
Here’s the basics of what happens where in the nephron.
Sodium ions are transported out as it water (which follows sodium). Hydrogen ions come in and interact with carbonic anhydrase which forms H2CO3 which is then converted to Hydrogen ions and HCO3 (bicarbonate).
Same as PCT above, but the DCT also secretes K+ (potassium) in exchange for Na+ (sodium ions). This is important because K+ secretion is controlled by aldosterone. There are aldosterone receptors here. This is important in terms of the Renin-Angiotensin-Aldosterone blood pressure connection.
Na+ is reabsorbed with Cl- which is actively absorbed and follows.
The result of all the above is the osmotic gradient along the nephron: more Na+ in blood and less in the renal tubules. Water molecules then migrate with the Na+ into the blood, mostly in the PCT and collecting ducts. ADH (antidiruretic hormone) causes the pores of the collecting ducts to open so water can follow the Na+. When there is less water in the urine there is lower urine volume. This maintains the plasma volume and water balance. Diuretics increase urine flow by inhibiting renal tubular reabsorption of Na+ and water. Conditions associated with renal dysfunction
☯ Nephritis is an inflammation or infection of renal tissues ☯ Glomerulonephritis ☯ Pyelonephritis ☯ CHF, circulatory problems, HTN, and shock all lower blood flow to kidneys and can produce
renal failure. Damage and other blood flow inhibition to renal tissue results in lowered urine
flow, volume or even anuria. When the blood is not filtered, toxins build up in the blood and can cause uremia, edema, and hypertension.
☯ Uremia/toxemia is the accumulation of nitrogenous wastes in the blood. ☯ Edema/HTN is fluid retention and accumulation in extracellular spaces with too much salt. This
causes an increase in blood volume and then hypertension.
Clinical indications for diuretics Diuretics manage anuria, HTN, and edema. Some stimulate urine production by increase glomerular filtration, some by reducing the amount of Na+ absorbed in the nephron. There are 5 major classes:
☯ Osmotic agents ☯ Thiazide and thiazide-like agents ☯ Carbonic anhydrate inhibitors ☯ Organic acids ☯ Potassium sparing
All cause diuresis by inhibiting the water/ Na+ reabsorption process in the kidneys. Osmotic diuretics These are filterable by the glomerulus but are not reabsorbed by the renal tubules. They become trapped in the tubular lumen and create an osmotic gradient. Water molecules follow the diuretics and both are excreted in the urine. There is no alteration of the sodium level and no change in the electrolyte or pH of the blood. Mannitol (Ocmitrol)
This is the most frequent one given. Can penetrate the cell membranes, but has to be given via IV. Used for anuria, oliguria, acute renal failure, in surgery for renal compromise patients, drug toxicity/overdose, cerebral edema, glaucoma, local swelling and edema with pressure. Adverse effects:
☯ N/D ☯ Chills ☯ Headache ☯ Strain on heart function due to increased blood plasma volume ☯ Contraindication: don’t use with chronic edema due to cardiac insufficiency.
Carbonic Anhydrase Inhibitors Acetazolamide/Diamox
Increases the levels of Na+ and water excreted by inhibiting carbonic anhydrase, so stops the hydrogen ions and bicarbonate ions from forming the PCT and DCT. Very little H+ is produced, so no Na+ is exchanged and therefore no water follows it out of the body. Note: since there is no sodium exchange in the DCT, it attempts to compensate by increasing the potassium exchange. This can cause a loss of calcium in the urine and eventually cause hypokalemia which affects the acid/base balance and can result in metabolic acidosis. This drug is not metabolized but is totally excreted by the kidney at the PCT to the urine.
☯ Treats edema due to CHF or drugs ☯ Functions on occular tissues lowering the pressure and edema of open or narrow angle
glaucoma because aqueous humor depends on carbonic anhydrase.
☯ Epilepsy. Acidosis decreases petit mal seizures and unlocalized seizures. ☯ Mountain sickness
*Hyperuricemia is too much uric acid in the body due to lowered urate excretion. This is especially problematic for gout patients. Contraindicated for:
☯ Patients with metabolic acidosis due to renal failure or respiratory acidosis ☯ Glaucoma patients with renal disturbance, depression or electrical imbalance.
Thiazide and thiazide-like diuretics This is the largest group. Both types have the same function on the tubules even though they aren’t necessarily chemically related. Cause diuresis by inhibiting sodium ions at the distal portions of the nephron causing sodium/water loss and intense diuresis. Also causes Cl- and K+ loss. This results in:
☯ Hypochloremic alkalosis ☯ Hypokalemia ☯ Hyponatremia (mostly in the elderly)
Diuresis will occur even with alkalosis. Drugs include:
*Hyperglycemia due to low glucose utilization. Use caution with diabetic patients.
Clinical indications: ☯ Immediate lowering of edema.
☯ Hypertension control due to lowered blood plasma levels, relaxation of the vascular smooth muscle.
Organic acid diuretics Organic acid diuretics work in the loop of Henle and promote diuresis by inhibiting sodium and chloride ions in the loop. This can also cause a loss of water along with the electrolytes, causing hypochloremic alkalosis. Because these drugs function despite pH changes in the blood hypokalemia is possible as well. Drugs include:
*Ototoxicity or tonedeafness is worse when combined with aminoglycoside antibiotics such as amikacin, kanamycin, neomycin, or streptomycin.
☯ Better effects than thiazides. Used for edema, especially when thiazides don’t work any longer. ☯ Severe peripheral edema and pulmonary edema. Includes edema due to CHF, liver cirrhosis, and
Potassium sparing diuretics These inhibit potassium at the DCT causing mild diuresis without electrolyte exchange or pH disturbance. Clinical indications:
☯ Edema. Combine with thiazides and loop diuretics (organic acids). ☯ Hyperaldosteronism – spironolactone specifically
Amiloride/Midamor
Inhibit sodium reabsorption by altering membranes at the DCT to keep potassium from excreting. Adverse effects:
☯ Nausea/diarrhea ☯ Hyperkalemia, esp with impaired renal function and in diabetics
Spironolactone/Aldactone
Blocks aldosterone receptors in the DCT thus inhibiting potassium exchange with sodium. Adverse effects:
☯ Nausea/diarrhea ☯ Hyperkalemia, esp with impaired renal function and in diabetics ☯ Gynecomastia
Triamterene/Dyrenium
Inhibit sodium reabsorption by altering membranes at the DCT to keep potassium from excreting. Adverse effects:
☯ Nausea/diarrhea ☯ Hyperkalemia, esp with impaired renal function and in diabetics ☯ Gynecomastia
Miscellaneous diuretics Xanthines, specifically. These include caffeine, Pamabrom, Theobromide, and Theophylline. All increase blood flow in the kidneys and have the side effects of CNS stimulation, hypotension, and headache. Drug interactions and incompatibilities Diuretics can bind to plasma proteins and alter pH by stimulating renal excretion. This means there’s a high potential for interaction with certain drugs or types of drugs.
Potential for toxicity as diuretics can induce hypokalemia which increases the toxic effects of digitalis and production of arrhythmias.
Diuretics decrease renal clearance of lithium increasing it’s toxicity.
Carbonic anhydrase inhibition causes potassium levels to decrease with corticosteroids causing a higher excretion of acidic drugs.
☯ Alcohol, antihypertensives, barbituates, opioids
Good possibility of orthostatic hypotension especially with thiazides and organic acids.
Orothotoxicity with organic acid diuretics.
Chapter 26
Blood pressure is determined by cardiac output and peripheral resistance. Cardiac output is calculated by heart rate X stroke volume. Peripheral resistance is the restistance/frication of the arterioles against blood flow and is increased by vasoconstriction. Vasoconstriction is affected by sympathetic stimulation (NOR and EPI), angiotensin, and other vasoactive factors. The kidneys also contribute to peripheral resistance. Resistance is higher in the kidneys than in the vascular areas. If renal blood flow falls due to hypertension the kidneys will release renin which prompts the production of angiotensin. Angiotensin prompts the adrenal cortex to release aldosterone which causes the kidneys to reabsorb more sodium ions and water increasing hydraulic pressure and blood pressure. Diuretics Diuretics work partially because they cause a reduction in blood volume due to diuresis. Thiazides also lower the sodium concentration in the blood vessel walls to there is less NOR/EPI action and less vasoconstriction. The result is vasodilation and a lower blood pressure. Diuretics can be used alone for mild HTN, but are combined with other drugs for moderate to severe HTN. Adverse effects:
☯ Loss of water, sodium and potassium ☯ Dehydration, fatigue and muscle weakness ☯ Uric acid increase means more gout attacks ☯ Because it interferes with insulin can cause hyperglycemia.
Sympathetic Blocking Drugs
Reduce the hyperactivity of the sympathetic nervous system and vasoconstriction, especially Clonidine which acts upon the medula oblongata vasomotor control. This lowers the level of sympathetic activity and increases vasodilation.
Dry mouth Constipation Drowsiness Withdrawl symptoms if not stopped gradually: headache, nausea, hypertensive
o Block beta 1 at the heart and lower cardiac output o Bloc release of renin at the kidney so that RAA (renin, angiotensin, aldosterone) cycle
stops. Propranolol has a central action in the CNS like clonidine and methyldopa for lowering blood pressure.
Vasodilators Act on vascular smooth muscle to cause relaxation. Usually combined with diuretics and beta blockers since vasodilator agents often causes fluid retention and tachycardia.
Moderate to severe HTN, used with diuretics and sympathetic blockers.
Nausea, vomiting Headache Reflex tachycardia Longterm use can cause rheumatoid arthritis, SLE type symptoms
More potent than hydralazine, used if patients don’t respond to vasodilators + diuretics + sympathetic blockers.
Myocardial ischemia Pericardial infusion Hirsuitism
(as a matter of fact, Rogaine is the topical form of this drug.)
Calcium ion antagonists These interfere with caldium ions transfering to smooth heart and vascular muscle which causes vasodilaton.
Déjà vu again. These are vasodilators and also depress the actions of the heart.
Only vasodilation. You’ll see some repeats here too. Note they all end in –dipine.
o Nifedipine o Nicardipine o Amlodipine (norvasc) o Felodipine (plendril) o Isradipine (dynacirc)
ACE inhibitors These stop the RAA cycle and dilate the vessels increasing renal blood flow. All end in –pril Adverse effects:
☯ Headaches ☯ Dizziness ☯ GI disturbances ☯ Rash ☯ Loss of taste sensation with captopril ☯ Rare: nonproductive cough or angioedema in the face and oral cavity.
Angiotensin receptor blockers Block angiotensin II receptors at the blood vessels and adrenal glands so no vasoconstriction or aldosterone release. Lowers sodium, lowers water retention and lowers blood pressure. All end in – sartan. Drugs include:
☯ Losartan (Cozaar) ☯ Candesartan (Atacand) ☯ Eprosartan (Teveten) ☯ Irbesartan (Micardis)
Adverse effects: None cause coughing or angioedema…
☯ Headache ☯ Dizziness ☯ GI disturbance
Hypertensive crisis This is sudden, severe HTN. 210/120 is malignant hypertension.
Similar to thiazide. Potent vasodilator, no diuretic action. IV. Lasts 6 – 12 hours. Can result in fluid retention, tacycardia and hyperglycemia.
Potent vasodilator for hypertensive emergencies. Short duration: 1 – 5 minutes.
International School Of Healing Arts Inspiring the Path of Health Join our list MARCH 2008 and receive a Greetings! Body Reading Poster !!! SPRING IS HERE! Wishing you all a fresh start for the new year. I will be teaching many classes and available for private sessions during April. I will be in Europe May through September Here are some of the late
 Chapter 21
Chapter 21 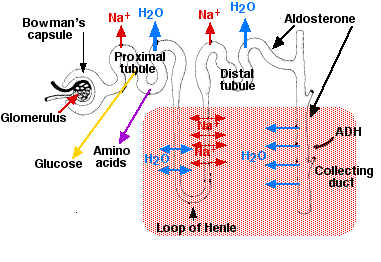 Any process interfering with this process then inteferes with the pH balance of the body. One example is acidosis, a result of insufficient bicarbonate production due to carbonic anhydrase inhibition. More on that soon. Normal cell metabolism produces uric acid, as well as other weak acids and bases. The PCT secretes weak acids/bases to the urine. A lot of drugs are also weak acids or bases and also secrete through the PCT to the urine. Metabolic waste products must then compete for the same realestate to get out of the body as the drugs do. This can result in altered drug excretion and accumulations of drugs or metabolic wastes in the body.
Here’s the basics of what happens where in the nephron.
Sodium ions are transported out as it water (which follows sodium). Hydrogen ions come in and interact with carbonic anhydrase which forms H2CO3 which is then converted to Hydrogen ions and HCO3 (bicarbonate).
Same as PCT above, but the DCT also secretes K+ (potassium) in exchange for Na+ (sodium ions). This is important because K+ secretion is controlled by aldosterone. There are aldosterone receptors here. This is important in terms of the Renin-Angiotensin-Aldosterone blood pressure connection.
Na+ is reabsorbed with Cl- which is actively absorbed and follows.
Any process interfering with this process then inteferes with the pH balance of the body. One example is acidosis, a result of insufficient bicarbonate production due to carbonic anhydrase inhibition. More on that soon. Normal cell metabolism produces uric acid, as well as other weak acids and bases. The PCT secretes weak acids/bases to the urine. A lot of drugs are also weak acids or bases and also secrete through the PCT to the urine. Metabolic waste products must then compete for the same realestate to get out of the body as the drugs do. This can result in altered drug excretion and accumulations of drugs or metabolic wastes in the body.
Here’s the basics of what happens where in the nephron.
Sodium ions are transported out as it water (which follows sodium). Hydrogen ions come in and interact with carbonic anhydrase which forms H2CO3 which is then converted to Hydrogen ions and HCO3 (bicarbonate).
Same as PCT above, but the DCT also secretes K+ (potassium) in exchange for Na+ (sodium ions). This is important because K+ secretion is controlled by aldosterone. There are aldosterone receptors here. This is important in terms of the Renin-Angiotensin-Aldosterone blood pressure connection.
Na+ is reabsorbed with Cl- which is actively absorbed and follows.