La spécificité du tadalafil est liée à sa longue demi-vie, permettant une action qui excède largement celle des autres inhibiteurs de PDE5. L’absorption digestive est complète, avec un pic plasmatique atteint en 2 heures environ. Le métabolisme est réalisé via CYP3A4, produisant des métabolites inactifs éliminés principalement dans les fèces. La sélectivité enzymatique est élevée, réduisant les effets indésirables extra-caverneux. Les réactions indésirables fréquentes incluent céphalées, bouffées vasomotrices et troubles digestifs légers. L’activité pharmacologique est stable, indépendamment de l’ingestion d’aliments. Dans les comparaisons de longue durée, acheter cialis pas cher est mentionné en relation avec les études portant sur la persistance d’efficacité et la constance de la cinétique plasmatique.
Premaks.tripod.com
Management of epistaxis in general practice Dennis Pashen, Maurice Stevens (Australian Family Physician, Vol 31, No 8, August 2002) Background. The vast majority of cases of epistaxis can be managed successfully within Objective. To describe a range of clinical interventions in the management of epistaxis Discussion. A number of relatively simple treatments and procedures may provide relief for
anterior nasal bleeding, which is the site for over 80% of cases of epistaxis. Where more procedural interventions are necessary, adequate preparation and appropriate tools are required to perform these procedures safely. Initial identification of the site of bleeding before commencement of treatment may be difficult but allows the correct treatment to be applied with minimal discomfort to the patient. More copious bleeding which constitutes less than 5-10% of cases, is usually the result of posterior nasal bleeding and is best treated in a facility well set up to handle such an eventuality. In cases of chronic epistaxis, a number of interventions, medical and surgical have been trialled with variable success, and should be used with caution in general practice.
The majority of cases of epistaxis arise from the nasal septum. Exceptions but not necessarily
exclusions to septal bleeding may occur with injury to the turbinates, congenital causes of bleeding such as hereditary haemorrhagic telangiectasia, blood dyscrasias, anticoagulation therapy, cardiovascular conditions including hypertension and raised venous pressure from mitral stenosis (Table 1). These are uncommon however.
The blood supply of the nasal septum is from the internal carotid through the anterior and
posterior ethmoidal arteries, and from the external carotid through greater palatine, sphenopalatine and superior labial arteries (Figure 1).
Some commonalities in epistaxis do exist however. It is messy for both the patient and
treating physician, and if copious, equally distressing.
Examination
Initial assessment can be delayed in acute epistaxis while immediate measures to stem the
tide are put in place. Direct digital pressure to the lower soft cartilaginous part of the nose by pinching for approximately 10 minutes is the method of choice. The patient should be sitting and leaning forward, breathing through the mouth and may suck on ice. This will allow time to prepare for the examination and protect your clothes, self, and the patient.
Once the initial flow has stemmed, the nasal cavity can be viewed. Persistence of bleeding
with adequate anterior control would suggest a more posterior origin of bleeding.
Light source
A good hands free light source is essential. A mirrored head loop, or a headlight that can be
focused. A Thudicum nasal speculum will allow viewing of the cavity. The sprung speculum is looped over the tip of the second finger, the back of the hand facing the patient, and is actively closed by compression using the third and fourth fingers. The speculum is inserted while closed, allowing the natural spring of the speculum to open up the anterior nares. A large calibre otic speculum and otoscope may also be used, but care must be taken during insertion into the nostril so as to not recommence any bleeding from the Little's area. This should allow ready access for small anterior septal bleeds necessary to perform cautery.
Table 1. Causes of epistaxis Local Causes
¾ Spontaneous: Little's area (anterior)
¾ Trauma: nasal fractures, septal ulcers, chronic perforations
¾ Tumours (benign and malignant), granulomas
General causes
¾ Raised venous pressure (mitral stenosis)
An effective suction device is necessary if the bleeding cannot be controlled. An angled
Fraser sucker, 10-12 French gauge, is preferred to allow evacuation of the anterior and middle nasal cavity.
Figure 1. Blood supply of nasal septum. Analgesia
Analgesia is most often not required in anterior cavity bleeding. Topical analgesia may be
required for posterior bleeding, especially if packing is required. A range of topical agents is available, either as packaged produces or prepared by a pharmacist. Sedation may be effective in bleeding that is a result of hypertension. Intramuscular morphine (0.05-0.15 mg/kg) or pethidine (0.5-1.5 mg/kg) have been used for many years and have proven to be of value. It is best to avoid narcotics until after control of haemorrhage. However, care must be taken to maintain airway safety in sedated patients. An intravenous lines should be inserted in the early treatment phase.
Local anaesthetic agents
¾ cophenylcaine forte (a mixture of xylocaine and decongestant) solution or spray
¾ xylocaine 10% solution with 1/10.000 adrenaline or xylocaine 10% CFC free spray
¾ xylocaine 2% 1/200.000 adrenaline ampoules for local injection
¾ cocaine 25$ in paraffin base ointment.
Equipment
A range of equipment may facilitate the treatment of epistaxis. This may include:
¾ Jobson Horne wool carrier, or long handled cottonbuds/swabs
¾ Foley's catheter, sponge foam stay, and clamp (from an intravenous line or umbilical
¾ angled rigid Fraser, 10-12 French gauge sucker
¾ triamcinolone ointment with and without antiseptic/antibiotic (Kenacomb ung). This is
also used following cautery to reduce crusting and hence reduce bleeding during healing.
Anterior epistaxis
Anterior epistaxis is the commonest form of epistaxis and constitutes over 80% of all cases
of epistaxis. Primarily this is the result of bleeding from the Little's area, which contains the Kiesselbach plexus of vessels (Figure 1). This is often triggered by infection to the overlying mucosa. In children, the ease with which small fingers can be inserted and the ensuing satisfaction that this provides contributes to a large number of cases, especially when associated with various organisms such as staphylococci and streptococci.
Figure 2. Electrocautery handpiece. Treatment
A conservative regimen can be trialled initially. A once a week application of Triamcinolone
0.025% cream (Aristocort cream), nemdyn, nasalate or equivalent cream combined with nightly application of a small quantity of petroleum jelly to the septum before bedtime.
Chemical cautery
Silver nitrate sticks can be applied over the Little's area. Topical anaesthetic may be applied
via spray or impregnated swabs before this.
Technique
Light application over the area of origin of bleeding may result in cauterisation of the
underlying vessels. This is achieved by lightly wiping the tip of the silver nitrate stick over the Little's area until it becomes discoloured to a grey-white. It may also trigger further bleeding. A clean cottonbud may be dabbed gently on the area to remove excess chemical or blood induced from rubbing. Caution must also be exercised in that ideally, only one side at a time should be cauterised by any means, as nasal septal perforation may result from bilateral cautery. Silver nitrate may stain
the skin of the nostril which can last for approximately three weeks. The patient shouldn't blow their nose for a few hours to avoid this happening (Figure 3).
Figure 3. Chemical cautery. Electrocautery
Electrocautery is performed after suitable anaesthesia such as topical anaesthetic followed by
local anaesthetic injection. The red-hot electrocautery loop is passed over the mucosal blood vessels effecting cautery (Figure 4). It must be noted that the cautery is achieved not by direct contact, but by the approximate application of heat, and that the anterior nares must be protected by a speculum or other means as burning can result in scarring. Topical antibiotic ointment and/or petroleum jelly can be used postoperatively.
Other forms of bleeding
In other forms of bleeding, obvious sites of haemorrhage may not be visualised. This may
include posterior bleeding from fractures or systemic causes, or injury to the turbinates. In cases of various systemic causes, tamponade via nasal catheters or packing provides the main treatment, at least initially.
Figure 4. Nasal electrocautery.
After application of topical and local anaesthetic (Figure 5, 6) packing can proceed with the
patient positioned sitting forward, holding a kidney tray, and breathing through his/her mouth. Adequate splash protection includes the wearing of plastic clothing covers, goggles or glasses, and gloves.
Figure 5. Lateral nerve supply of nose. Balloon catheters
Double balloon catheters, although expensive are easy to insert. After fully inserting the
catheter, the posterior balloon is first inflated and brought forward to close off the postnasopharyngeal space. The second and anterior balloon is then inflated to apply pressure to the internal cavity of the nose. Normal saline is the preferred agent for inflation of the balloons as gradual deflation can occur if air is used, and this may result in recurrence of bleeding. Do not inflate beyond the capacity of the balloons as discomfort, rupture of the balloons, or pressure necrosis of the mucosa may occur.
Figure 6. Anterior view of nerve supply of nose. Nasal packing (anterior and posterior bleeds) Preparation of the pack
A six foot strip of Vaseline gauze is placed into a surgically clean bowl and mixed with
triamcinolone and antibiotic cream (Kenacomb ointment). Many alternate mixtures exist, such as paraffin plus neotracin, or the traditional bismuth and iodoform paraffin paste (BIPP).
Anaesthesia
The patient's nose should be adequately anaesthetised, although it may be difficult. a good
headlamp and suction is necessary to clear any blood from the airway. Using cophenylcaine or cocaine spray or swabs, the nasal mucosa is anaesthetised as much as possible. The use of parenteral premedication or sedation should be used with caution as it is possible to tip the patient over into hypovolemic shock if blood loss has been severe.
Technique
A Foley's catheter with a foam stay placed on its proximal end is inserted along the floor of
the nasal cavity under the inferior turbinate, to the nasopharynx. The part of the catheter beyond the balloon may be removed to facilitate positioning and improve patient comfort. The pharynx is viewed to make sure the catheter has not passed into the oropharynx. The catheter balloon is then inflated with up to 8 mLs of normal saline, and should be no larger than the size of the choana (the posterior nasal aperture), and then brought forward by gentle traction.
At this stage there should be no blood in the pharynx if the choana is obstructed and the
catheter is on the correct side. The prepared pack is picked up in a loop, the length of which should be the length of the packing forceps, which is approximately equivalent to the length of the floor of the nose (Figure 7a, b). The loop is inserted inferiorly to the Foley's catheter, and subsequent loops placed above these parallel to one another and the floor of the nose (Figure 7c). The catheter needs to be fixed in position by the piece of foam being applied to the alar margin; this prevent any erosion of that margin. A suitable clamp is used to fix the stay in place (Figure 7d). This may be an intravenous line or an umbilical clamp, the former preferable, as it is more easily adjustable. The tension on the catheter should be sufficient to keep it in place but not enough to interfere with the viability of the skin of that region. The pack can then be left in place for one to three days which is necessary to stabilise the haemostasis. Often the tension on the catheter is released after 24 hours but the catheter is left in place.
Figure 7a, b, c, d. Foley's catheter. Continuing bleeding
A range of medical and surgical interventions is required in cases of continuing and/or severe
bleeding. These are best delivered within the context of a specialist unit in a tertiary hospital as often resuscitation may be required. Such medical interventions as intravenous administration of Tranexamic Acid, 0.5-1.0 gm four times a day in hereditary haemorrhagic telangiectasia, ligation of internal or external carotids are not for the faint-hearted and are best left to major centres.
Conclusion
Epistaxis is a common presentation with over 60% of the population suffering from it at
some stage of their lives. It is often influenced by environmental conditions. Over 80% of these are attributable to anterior nasal cavity causes. The general practitioner may be required to deal with this condition and can do so in the majority of cases in an appropriate and safe manner. With training and knowledge they may also be able to take appropriate measures to deal with other causes of bleeding.
Further guidance and reading
¾ Upya nose, Inya Ear and Downya throat. CD-ROM available from the RACGP library,
NQ Clinical School, Mt Isa Health Service District Library, or the author.
¾ Hamilton Bailey's Emergency Surgery. Butterworth-Heinemann, Linnacre House, Jordan
Hill, Oxford OX2 8DP. ISBN 0 7506 2771 9.
Summary of Important Points
¾ The majority of cases of epistaxis originate from the anterior septal area (Little's area).
¾ Chemical cautery (silver nitrate) and electrocautery are treatments of choice for anterior
epistaxis and can be delivered with minimal discomfort and cost in general practice.
¾ Adequate preparation includes having the appropriate equipment to enable easy and
¾ Nasal packing is appropriate management for posterior and recalcitrant epistaxis. Adequate analgesia is mandatory. Packing can be performed in a well-equipped general
¾ Do not forget that patients can die from epistaxis. Attention to normal resuscitation
Reprint Requests Dennis Pashen Mt Isa Centre for Rural and Remote Health PO Box 2572 Mt Isa, Qld 4825 Email: [email protected]
Hinweise zur Interpretation von Sortenversuchsergebnissen und Empfehlungen zur Sortenwahl bei Mais VOLKER MICHEL Gesamtbewertung und Sortenempfehlung Silomais Zur Gesamtbewertung der Sorten ist beim Silomais die komplexe Interpretation der Eigen-schaften und Zusammenhänge von Ertrag, Reife, Energiekonzentration der Gesamtpflanze, Stärkeertrag (indirekt auch Stärkegehalt) sowie
Aspectos generAles El consumo de bebidas alcohólicas supone una práctica frecuente en la sociedad contemporánea. Según el último estudio domiciliario sobre el uso de drogas psico-trópicas en Brasil, realizado por el Centro Brasileño de Información sobre Drogas Psicotrópicas del Departamento de Psicobiología de la Universidad Federal de São Paulo (Cebrid/Unifesp),1 un 74,6% de los br
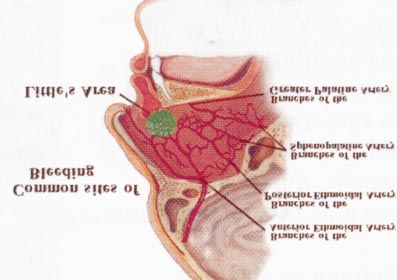 Figure 1. Blood supply of nasal septum.
Figure 1. Blood supply of nasal septum. 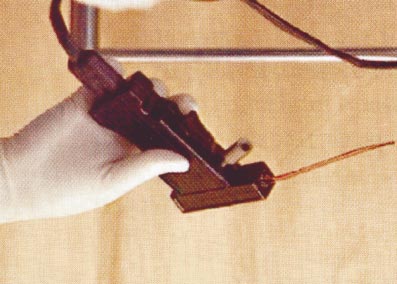 also used following cautery to reduce crusting and hence reduce bleeding during healing.
Anterior epistaxis
also used following cautery to reduce crusting and hence reduce bleeding during healing.
Anterior epistaxis 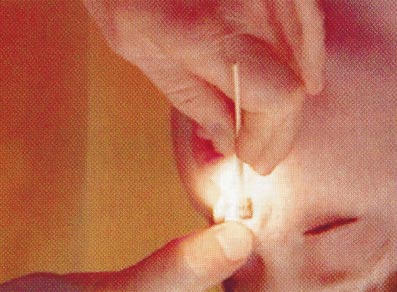 the skin of the nostril which can last for approximately three weeks. The patient shouldn't blow their nose for a few hours to avoid this happening (Figure 3).
Figure 3. Chemical cautery.
the skin of the nostril which can last for approximately three weeks. The patient shouldn't blow their nose for a few hours to avoid this happening (Figure 3).
Figure 3. Chemical cautery. 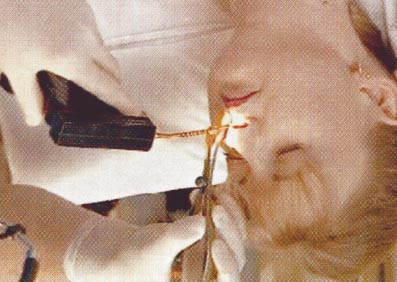
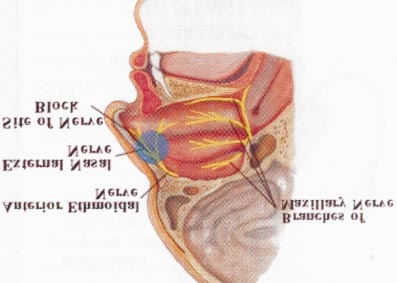 Figure 4. Nasal electrocautery.
Figure 4. Nasal electrocautery. 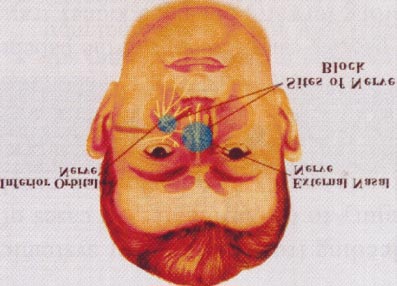 Balloon catheters
Balloon catheters 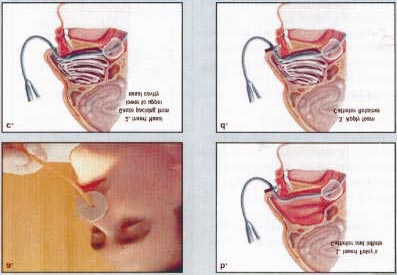 Technique
Technique