La spécificité du tadalafil est liée à sa longue demi-vie, permettant une action qui excède largement celle des autres inhibiteurs de PDE5. L’absorption digestive est complète, avec un pic plasmatique atteint en 2 heures environ. Le métabolisme est réalisé via CYP3A4, produisant des métabolites inactifs éliminés principalement dans les fèces. La sélectivité enzymatique est élevée, réduisant les effets indésirables extra-caverneux. Les réactions indésirables fréquentes incluent céphalées, bouffées vasomotrices et troubles digestifs légers. L’activité pharmacologique est stable, indépendamment de l’ingestion d’aliments. Dans les comparaisons de longue durée, acheter cialis pas cher est mentionné en relation avec les études portant sur la persistance d’efficacité et la constance de la cinétique plasmatique.
Untitled
Decreased gyrification in major depressive disorderYuanchao Zhanga,b, Chunshui Yuc, Yuan Zhoub,d, Kuncheng Lic, Chong Lia,band Tianzi Jiangb
Structural and functional abnormalities have been extensively
reported in major depressive disorder, but possible changes in
Keywords: complexity, connectivity, cortical folding, local gyrification index,
cortical folding have not yet been explored in this disorder.
magnetic resonance imaging, major depressive disorder
This study investigated this issue in major depressive disorder
using the local gyrification index. High-resolution magnetic
aDepartment of Mathematics, Zhejiang University, Hangzhou, bNational
resonance imaging was performed in 18 patients with first-
Laboratory of Pattern Recognition, Institute of Automation, Chinese Academyof Sciences, cDepartment of Radiology, Xuanwu Hospital of Capital Medical
episode major depressive disorder and 18 age-matched and
University and dCenter for Social and Economic Behavior, Institute of Psychology,
sex-matched healthy individuals. The local gyrification index
Chinese Academy of Sciences, Beijing, PR China
was applied to detect brain areas with abnormal corticalfolding in major depressive disorder. Compared with healthy
Correspondence to Professor Tianzi Jiang, PhD, National Laboratory of Pattern
participants, patients with major depressive disorder showed
Recognition, Institute of Automation, Chinese Academy of Sciences, Beijing100190, PR China
significantly decreased local gyrification index in the bilateral
Tel: + 86 10 8261 4469; fax: + 86 10 62551993; e-mail: [email protected]
mid-posterior cingulate, insula, and orbital frontal cortices, theleft anterior cingulate cortex, and the right temporal
Yuanchao Zhang, Chunshui Yu, and Yuan Zhou contributed equally to this study
Kluwer Health | Lippincott Williams & Wilkins.
Received 28 November 2008 accepted 30 November 2008
Major depressive disorder (MDD) is a common psychiatric
Eighteen medication-naive patients with first major
overwhelming feelings of sadness, guilt, and worthlessness.
depressive episode (four men and 14 women) were
It is believed that depression is related to the disturbance
recruited from the outpatient clinic at Xuanwu Hospital
in connectivities between multiple brain regions [1].
and met the following criteria: (i) Diagnostic and Statistical
This opinion is supported by abnormalities in both
Manual of Mental Disorders 4th edition criteria for a major
cortico–cortical connectivity revealed by disrupted white
depressive episode, single episode, currently depressed,
according to the structured clinical interview for
revealed by gial cell pathology in MDD [3–5]. Cortical
Diagnostic and Statistical Manual of mental disorders
folding, which can be investigated by gyrification
fourth edition; (ii) never exposure to any psychotropic
measures, is thought to reflect not only cortico–cortical
medication before the assessment began; (iii) age 18–60
connectivity [6] but also optimal intracortical organiza-
years; (iv) no history of substance abuse or dependence,
tion, with the most axonal connections in the least
no family history of major psychiatric or neurological
possible volume [7]. Therefore, investigating the pattern
illness in first-degree relatives, not currently taking any
of cortical folding in MDD patients may contribute in
prescription or centrally acting medications, no serious
understanding the pathogenesis of the disorder.
medical or neurological illness; and (v) satisfying thecriteria to undergo a magnetic resonance imaging (MRI)
The gyrification index (GI) proposed by Zilles et al. [8] is
scan based on a MRI screening questionnaire. The
a quantitative measure of gyrification, but this method is
patients were excluded for any axis I disorder (other
rater dependent and cannot localize the exact regions
than MDD) that preceded the onset of MDD. Additional
with abnormal cortical folding. The local gyrification
exclusion criteria were as follows: acutely suicidal or
index (lGI), a three -dimensional extension of GI, is
homicidal or requiring inpatient treatment, history of
a newly developed, automated method for locating
trauma resulting in loss of consciousness, current
regionally specific changes in gyrification, and has been
pregnancy, or breastfeeding. At the time of scanning,
successfully used to assess gyrification of the 22q11
the depressive symptoms of the patients were rated using
Deletion syndrome [9]. In this study, we use this measure
to explore gyrification abnormalities in MDD.
(17.8 ± 3.6). Eighteen demographically matched healthy
c 2009 Wolters Kluwer Health | Lippincott Williams & Wilkins
participants (four men and 14 women) were recruited by
advertisements and met the same inclusion criteria (iii–v)and the exclusion criteria as the patients. All participantstook part in this study after signing an informedconsent form approved by the Medical Research Ethics
Committee of Xuanwu Hospital. The mean duration ofcurrent depressive episode of MDD patients was
6.7 ± 3.9 months. All patients were on no antidepressantmedications at the time of scanning. The two groups
were statistically comparable in age (39.8 ± 9.3 years forMDD;
P=0.8173) and sex composition (P=1).
Three-dimensional structural MRI scans were obtained on a3.0 Tesla magnetic resonance scanner (Trio system; Siemens
Brain regions of significantly decreased local gyrification index in
Magnetom scanner, Erlangen, Germany) with magnetization
patients with major depressive disorder compared with well-matched
prepared rapid acquisition gradient echo (MP-RAGE).
healthy participants after a correction for multiple comparisons(P < 0.05, the cluster-based random field theory correction). The color
Detailed scan parameters were as follows: repetition
bar indicates the cluster-wise P value after the correction for multiple
time = 2000 ms, echo time = 2.6 ms, slice thickness = 1 mm,
no gaps, flip angle = 91, matrix = 256 Â 224, field ofview = 256 Â 224 mm2, 1 Â 1 mm2 in-plane resolution.
clusters was set at P value of less than 0.05 after multiple
Each scan was processed using FreeSurfer [10,11] (http://
surfer.nmr.mgh.harvard.edu/) to obtain the complexitymeasure (lGI). In brief, a cortical map of lGIs can be
obtained in four steps [9]. First, the pial cortical surface is
Only decreased lGI was found in MDD patients
reconstructed in three-dimensional space. Second, an
compared with healthy participants. We found nine
outer surface can be obtained from the outer hull that
clusters of difference with thresholds of P=0.001
tightly warps the pial surface. Third, the lGI is computed
(uncorrected) and cluster size Z 50 points. These
for each of the vertices of the outer surface. Fourth,
clusters included the bilateral mid-posterior cingulate,
a cortical map of lGIs is obtained by propagating the
insula, and orbital frontal cortices, the left anterior
lGI values from the outer surface mesh to the pial
cingulate cortex, and the right temporal operculum. After
performing multiple comparison correction using randomfield theory , we identified five significant clusters, which
To compare the lGIs point by point, the establishment
included the left insular/frontal operculum (cluster
of point correspondence across participants in a standard
size=2184 points, corrected P value=0.0039), the left
surface-based coordinate system was required. Surface-
medial orbital frontal cortex (cluster size=1907 points,
based registration [12] was used to build an average
corrected P value=0.0021), the left mid-posterior
template and all of the individual reconstructed cortical
cingulate cortex (cluster size=1041 points, corrected
surfaces were aligned to the template. A heat kernel of
P value=0.0428), the right insula/temporal operculum
10 mm width was used to smooth the lGI maps. Before
(cluster size=1471 points, corrected P value=0.0113),
the statistical analysis, a linear regression was performed
and the right inferior frontal gyrus (cluster size=303
to remove the effects of age and sex. The residuals of the
points, corrected P value=0.0444) (Fig. 1).
regression were used for statistical analysis.
In this study, we used a surface-based approach to
Statistical analysis was performed at every point across all
quantify the local cortical gyrification in well-matched
participants in Montreal Neurological Institute space.
samples of MDD patients versus healthy participants.
Two-sample t-tests were used to test statistically
We revealed decreased gyrification in MDD patients
significant differences in lGIs at homologous vertices.
compared with healthy participants in certain mood-
The threshold P=0.001 was used to define clusters, and
only clusters with a minimum of 50 points were reported. Then corrected cluster-wise P value was obtained using
There are several possible explanations for the decreased
random field theory [13]. The level of significance for
Decreased gyrification in MDD Zhang et al.
A mechanical model of brain convolutional development
has been used to explain abnormalities in cortical folding
In conclusion, we found decreased gyrification in several
during human brain development [14]. This model
mood-related regions in patients with MDD compared
proposes that differential growth rates of cortical layers
with healthy participants. To our knowledge, this is the
directly affect the degree of cortical convolutions. In fact,
first study to explore the cortical folding pattern in MDD.
several previous studies have found decreased glial
Further studies are needed to clarify the exact mechanism
density, neuronal density, and neuronal size in several
of the abnormal cortical folding in MDD.
mood-related regions such as the anterior cingulatedcortex [4] and the orbitofrontal cortex [3,5] in MDD.
Therefore, the decreased gyrification in the mood-relatedregions might be caused by disorganization of the cortical
The authors thank Marie Schaer, Lei Lin, Kun Wang for
architectures in these regions. Another tension-based
their useful suggestions and Jiefeng Jiang, Yongfu Hao,
model of cortical morphogenesis proposes that tension
Professor Keith J. Worsley for their help on the artwork.
along the axons in white matter is the primary driving
The authors also thank Dr Edmund F. and Dr Rhoda E.
force for cortical folding [6]. In MDD, previous diffusion
Perozzi for checking the English. This work was supported by
tensor imaging studies have revealed that depressive
the Natural Science Foundation of China, grant no.
patients had a significantly lower fractional anisotropy
30425004, 30670601, 30870694, and 30730035, and the
in the prefrontal white matter [2]. In addition, in
National Key Basic Research and Development Program
previous diffusion tensor imaging studies, white matter
abnormalities of the anterior cingulated cortex, theprefrontal lobe, the insula, and the posterior cingulate
regions have been reported in patients with geriatric
Mayberg HS. Modulating dysfunctional limbic-cortical circuits in depression:
depression [15–17]. According to the tension-based theory
towards development of brain-based algorithms for diagnosis and optimisedtreatment. Br Med Bull 2003; 65:193–207.
of cortical morphogenesis, the decreased gyrification might
Li L, Ma N, Li Z, Tan L, Liu J, Gong G, et al. Prefrontal white matter
be because of the abnormal connectivity caused by white
abnormalities in young adult with major depressive disorder: a diffusion
matter abnormalities in these regions.
tensor imaging study. Brain Res 2007; 1168:124–128.
Cotter D, Mackay D, Chana G, Beasley C, Landau S, Everall IP. Reducedneuronal size and glial cell density in area 9 of the dorsolateral prefrontalcortex in subjects with major depressive disorder. Cereb Cortex 2002;
The hypothesis that MDD is of neurodevelopmental origin
Cotter D, Mackay D, Landau S, Kerwin R, Everall I. Reduced glial cell density
has been proposed recently. In the neurodevelopmental
and neuronal size in the anterior cingulate cortex in major depressive
perspective, MDD is considered to result from a combination
disorder. Arch Gen Psychiatry 2001; 58:545–553.
of genetic and harmful environmental factors during the
Rajkowska G, Miguel-Hidalgo JJ, Wei J, Dilley G, Pittman SD, Meltzer HY,et al. Morphometric evidence for neuronal and glial prefrontal cell pathology
developmental process [18]. Studies have shown that both
in major depression. Biol Psychiatry 1999; 45:1085–1098.
environmental and genetic factors may have an effect on
Van Essen DC. A tension-based theory of morphogenesis and compact
the patterns of cortical folding. For example, sheep
wiring in the central nervous system. Nature 1997; 385:313–318.
Klyachko VA, Stevens CF. Connectivity optimization and the positioning of
fetuses, which were exposed to short periods of mid-
cortical areas. Proc Natl Acad Sci U S A 2003; 100:7937–7941.
gestation hypoxi,a showed significantly reduced surface
Zilles K, Armstrong E, Schleicher A, Kretschmann HJ. The human pattern of
folding index compared with controls [19]. In addition,
gyrification in the cerebral cortex. Anat Embryol (Berl) 1988; 179:173–179.
Schaer M, Cuadra MB, Tamarit L, Lazeyras F, Eliez S, Thiran JP. A surface-
a study on the human brain has shown that mutations in
based approach to quantify local cortical gyrification. IEEE Trans Med
GPR56, which encodes an orphan G protein-coupled
receptor, can cause a cortical malformation called bilateral
Dale AM, Fischl B, Sereno MI. Cortical surface-based analysis. I. Segmentation and surface reconstruction. NeuroImage 1999; 9:179–194.
frontoparietal polymicrogyria [20]. In the perspective of
Fischl B, Sereno MI, Dale AM. Cortical surface-based analysis. II: Inflation,
neuroplasticity, environmental factors have been shown
flattening, and a surface-based coordinate system. NeuroImage 1999;
to influence the morphology of brain circuits during
Fischl B, Sereno MI, Tootell RB, Dale AM. High-resolution intersubject
adulthood. For example, in a study about the impact of
averaging and a coordinate system for the cortical surface. Hum Brain Mapp
chronic stress on the brain of rat [21], researchers found
that chronic stress can alter dendritic morphology in
Hayasaka S, Phan KL, Liberzon I, Worsley KJ, Nichols TE. Nonstationarycluster-size inference with random field and permutation methods.
medial prefrontal cortex, which is an important part of
limbic-thalamic-cortical circuits. In addition, another
Caviness VS Jr. Mechanical model of brain convolutional development.
study reported that chronic stress can inhibit cell
Science (New York, NY) 1975; 189:18–21.
Alexopoulos GS, Murphy CF, Gunning-Dixon FM, Latoussakis V,
proliferation in medial prefrontal cortex of adult rat, and
Kanellopoulos D, Klimstra S, et al. Microstructural white matter abnormalities
this suppressive effect of stress can be reversed by
and remission of geriatric depression. Am J Psychiatry 2008;
antidepressant treatment [22]. Therefore, it is possible
Taylor WD, MacFall JR, Payne ME, McQuoid DR, Provenzale JM, Steffens DC,
that abnormalities in genetic and/or environmental factors
et al. Late-life depression and microstructural abnormalities in dorsolateral
during the developmental process and adulthood may
prefrontal cortex white matter. Am J Psychiatry 2004; 161:1293–1296.
contribute to the decreased gyrification in mood-related
Yuan Y, Zhang Z, Bai F, Yu H, Shi Y, Qian Y, et al. White matter integrity ofthe whole brain is disrupted in first-episode remitted geriatric depression.
Ansorge MS, Hen R, Gingrich JA. Neurodevelopmental origins of depressive
Czeh B, Perez-Cruz C, Fuchs E, Flugge G. Chronic stress-induced cellular
disorders. Curr Opin Pharmacol 2007; 7:8–17.
changes in the medial prefrontal cortex and their potential clinicalimplications: does hemisphere location matter? Behav Brain Res 2008;
Rees S, Stringer M, Just Y, Hooper SB, Harding R. The vulnerability of the fetal
sheep brain to hypoxemia at mid-gestation. Brain Res 1997; 103:103–118.
Czeh B, Muller-Keuker JI, Rygula R, Abumaria N, Hiemke C, Domenici E,
Piao X, Hill RS, Bodell A, Chang BS, Basel-Vanagaite L, Straussberg R,
et al. Chronic social stress inhibits cell proliferation in the adult medial
et al. G protein-coupled receptor-dependent development of human frontal
prefrontal cortex: hemispheric asymmetry and reversal by fluoxetine
cortex. Science (New York, NY) 2004; 303:2033–2036.
treatment. Neuropsychopharmacology 2007; 32:1490–1503. LIPPINCOTT WILLIAMS and WILKINS JOURNAL NAME: WNR ARTICLE NO: QUERIES AND / OR REMARKS Details Required Author's Response
PROGRAMA FINAL III Curso Internacional sobre Obesidad en Español SAN ANTONIO, TEXAS 2009 TEMAS SELECTOS Avances en: Aspectos de Fisiología y Bioquímica Aplicados a la Clínica en el Manejo de la Obesidad Aspectos Genómico -Moleculares para Entender la Biología del Tejido Adiposo Estado del Arte 2009 RAUL A. BASTARRACHEA, M.D. Profesor Ti
Public Health Fact Sheet RED TIDE (Paralytic Shellfish Poisoning) What is Red Tide? Red Tide is caused by a "population explosion" of toxic, naturally occurring microscopic plankton (specifically, a subgroup known as dinoflagellates). "Blooms" of the poison-producing plankton are coastal phenomena caused by environmental conditions, which promote explosive growth. Fa
 Decreased gyrification in major depressive disorderYuanchao Zhanga,b, Chunshui Yuc, Yuan Zhoub,d, Kuncheng Lic, Chong Lia,band Tianzi Jiangb
Structural and functional abnormalities have been extensively
reported in major depressive disorder, but possible changes in
Keywords: complexity, connectivity, cortical folding, local gyrification index,
cortical folding have not yet been explored in this disorder.
Decreased gyrification in major depressive disorderYuanchao Zhanga,b, Chunshui Yuc, Yuan Zhoub,d, Kuncheng Lic, Chong Lia,band Tianzi Jiangb
Structural and functional abnormalities have been extensively
reported in major depressive disorder, but possible changes in
Keywords: complexity, connectivity, cortical folding, local gyrification index,
cortical folding have not yet been explored in this disorder.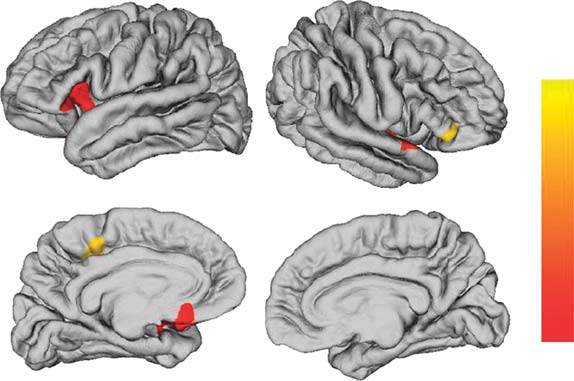 participants (four men and 14 women) were recruited by
advertisements and met the same inclusion criteria (iii–v)and the exclusion criteria as the patients. All participantstook part in this study after signing an informedconsent form approved by the Medical Research Ethics
Committee of Xuanwu Hospital. The mean duration ofcurrent depressive episode of MDD patients was
6.7 ± 3.9 months. All patients were on no antidepressantmedications at the time of scanning. The two groups
were statistically comparable in age (39.8 ± 9.3 years forMDD;
P=0.8173) and sex composition (P=1).
participants (four men and 14 women) were recruited by
advertisements and met the same inclusion criteria (iii–v)and the exclusion criteria as the patients. All participantstook part in this study after signing an informedconsent form approved by the Medical Research Ethics
Committee of Xuanwu Hospital. The mean duration ofcurrent depressive episode of MDD patients was
6.7 ± 3.9 months. All patients were on no antidepressantmedications at the time of scanning. The two groups
were statistically comparable in age (39.8 ± 9.3 years forMDD;
P=0.8173) and sex composition (P=1).