La spécificité du tadalafil est liée à sa longue demi-vie, permettant une action qui excède largement celle des autres inhibiteurs de PDE5. L’absorption digestive est complète, avec un pic plasmatique atteint en 2 heures environ. Le métabolisme est réalisé via CYP3A4, produisant des métabolites inactifs éliminés principalement dans les fèces. La sélectivité enzymatique est élevée, réduisant les effets indésirables extra-caverneux. Les réactions indésirables fréquentes incluent céphalées, bouffées vasomotrices et troubles digestifs légers. L’activité pharmacologique est stable, indépendamment de l’ingestion d’aliments. Dans les comparaisons de longue durée, acheter cialis pas cher est mentionné en relation avec les études portant sur la persistance d’efficacité et la constance de la cinétique plasmatique.
The lack of efficacy of different infusion rates of intrathecal baclofen in complex regional pain syndrome: a randomized, doubleblind, crossover study
Pain Medicine 2011; 12: 459–465Wiley Periodicals, Inc.NEUROPATHIC PAIN SECTION Original Research Article The Lack of Efficacy of Different Infusion Rates of Intrathecal Baclofen in Complex Regional Pain Syndrome: A Randomized, Double-Blind, Crossover Studypme_1065459.465 Anton Adriaan van der Plas, MD,* Johan Marinus, Results. There were no significant differences PhD,* Sam Eldabe, MD,† Eric Buchser, MD,‡ and between the FIRD and the SIRD groups for the Jacobus Johannes van Hilten, MD, PhD* median change of numeric rating scale dystonia (–0.3 [interquartile range {IQR} -1.1–0.5]), pain (0.1
*Department of Neurology, Leiden University Medical
[IQR –0.8–1.3]), and secondary outcomes, except for the frequency of adverse events, which was signifi- cantly higher during FIRD (12 vs 2). FIRD was pre- ferred only by patients who were included because
Department of Pain and Anaesthesia, James Cook
side effects to ITB prevented dose escalation.
University Hospital, Middlesbrough, England, UK;
Conclusions. Increasing the IR at a fixed daily dose
‡Pain Clinic, Morges Hospital, Morges, Switzerland
is not associated with improvement of dystonia or pain but warrants further investigation in patients in Reprint requests to: Anton A. van der Plas, MD,
whom side effects prevent further dose escalation.
Department of Neurology, Leiden University MedicalCenter, P.O. Box 9600, 2300 RC Leiden, The
Key Words. Infusion; Rate; Intrathecal; Baclofen;
+31-71-524-8253; E-mail: [email protected]. Introduction Abstract
Complex regional pain syndrome type I (CRPS I) is com-
Objective. Intrathecal baclofen (ITB) is effective in
monly preceded by injury, usually to a limb, and is char-
the treatment of dystonia related to complex
acterized by pain, disturbed blood flow, temperature
regional pain syndrome (CRPS). In a previous study,
regulation, and motor control of the affected area [1–3]. we noted that the responsiveness to ITB declined in
Approximately 20% of patients with CRPS develop dys-
30% of patients once drug delivery was switched
tonia, which is characterized by fixed flexion postures
from an external to an implanted device associated
[1,4–7]. Because dystonia in CRPS tends to spread to
with a reduction of the infusion rate (IR).
other limbs, the syndrome may evolve into a disablingdisorder with a marked impact on quality of life [4,6,8]. Design. In a double-blind study, we investigated the
Impaired inhibitory control of sensorimotor circuits is a key
effect of varying the IR at a fixed daily dose on the
pathophysiological finding in dystonia of CRPS [9]. efficacy and safety of ITB in patients with CRPS-
Baclofen stimulates pre- and postsynaptic gamma-
related dystonia. Patients were randomized to either
aminobutyric acid B receptors, which enhances central
slower infusion rate delivery (SIRD) or four-times
inhibitory activity [10,11]. However, dystonia in CRPS is
faster infusion rate delivery (FIRD) for 2 weeks and
rarely controlled by oral baclofen, probably because of the
were crossed over after a 1-week washout period.
drug’s poor ability to pass the blood–brain barrier [12,13];although in some patients, beneficial effects are reported
Patients. Patients were eligible if they experienced
with dosages as high as 90–120 mg/day [4]. Epidural
no beneficial response to ITB on dystonia despite a
administration of baclofen was shown to be beneficial in
minimum dose of 600 mg/day, or because side
intractable spasticity likely because the drug is lipid
effects limited dose escalation.
soluble and may cross the dura to act on the spinal canal[14]. Intrathecal delivery of baclofen overcomes the
Outcome Measures. Primary outcome measures
obstacle of the blood–brain barrier and results in greater
were changes in global dystonia and pain severity.
therapeutic efficacy concentrated at the spinal site of
van der Plas et al.
Drug delivery characteristics during screening procedure and post-pump implantation [16]
IQR = interquartile range; ITB = intrathecal baclofen.
action [15,16]. However, not all patients may respond to
and the study was approved by the local Ethics Commit-
this mode of drug delivery, which is expensive and
tee. The trial was registered in The Netherlands National
requires an invasive implantation procedure. Hence, a
Trial Register (NTR 1269). All patients were followed in our
screening procedure with an external pump is frequently
outpatient clinic and had CRPS-related dystonia in at least
used to evaluate the responsiveness to intrathecal
one extremity for which continuous ITB was administered.
baclofen (ITB) to help select those patients that are most
The patients fulfilled the CRPS criteria of the International
suitable for continuous ITB delivery through an implanted
Association for the Study of Pain including continuing
pump. Against this background, we screened patients
pain; allodynia or hyperalgesia disproportionate to any
using a 2-day placebo run-in dose escalation (200–
inciting event; evidence at some time of edema; changes
800 mg ITB) design [16]. The responder criterion for pump
in skin blood flow or abnormal sudomotor activity in the
implantation was set at a Ն25% improvement of global
area of pain; and the absence of any condition that would
dystonia severity on two consecutive baclofen days as
otherwise account for the degree of pain and dysfunction
compared with placebo. However, after pump implanta-
[2]. Patients had received an internal programmable Syn-
tion, 30% of patients on ITB surprisingly failed to meet the
chromed EL or II® pump (Medtronic, Minneapolis, MN,
responder criterion of the screening despite the use of a
USA) for continuous infusion of ITB after oral baclofen up
minimum daily dose of 600 mg or because side effects
to a minimal daily dose of 60 mg failed to provide benefi-
limited dose escalation. In an attempt to find an explana-
cial response or side effects limited escalation of the daily
tion for this finding, we reviewed the procedures of our
dose [16]. Patients were eligible for the IR study if they
study [16]. We found that the infusion rates (IRs) applied
experienced no beneficial response to ITB on dystonia at
during the screening and postimplantation period differed
a minimum daily dose of 600 mg, or dose-limiting side
because of the use of different baclofen concentrations
effects prohibited dose escalation of ITB. Furthermore,
(0.5 mg/mL vs 3 mg/mL) (Table 1). The IRs decreased
patients had to rate their global dystonia severity as at
once patients were switched to 3 mg/mL concentration in
least 5 on a numeric rating scale (NRS) ranging from 0
the postimplantation period. Two different concentrations
(absent) to 10 (most severe) in order to be eligible for the
were used because of the utilization of two pumps with
study. Exclusion criteria were identical to those used in a
different requirements for effective drug delivery. Could the
previous study examining the efficacy of ITB in CRPS-
lack of response to ITB in some patients, after the switch
related dystonia [16]. In 11 patients, a screening proce-
to the higher baclofen concentration, be explained by the
dure was performed using an external microinfusion pump
use of lower IRs? In an animal model, higher IRs of
before pump implantation [16]. The remaining three
baclofen and bupivacaine increased the drug’s cere-
patients participated in a trial with intrathecal glycine, after
brospinal fluid distribution; although experiments were
which they were switched to ITB without a screening
performed in a nonphysiological setting [17] and pain
procedure [19]. These three patients were included in this
severity was reduced by increasing the IR of intrathecally
study because they failed to improve Ն25% in dystonia
delivered bupivacaine in patients with intractable pain [18].
severity as a result of dose-limiting side effects to ITB.
To our knowledge, the influence of the IR on the clinical
Pump-catheter system integrity was verified in all patients
efficacy of ITB, independent of the daily dose, has not
prior to the study, and other conditions potentially influ-
been described to date. In this study, we compared the
encing dystonia severity were ruled out. At baseline, the
efficacy and safety of two ITB IRs at a fixed daily dose in
administered daily dose varied between patients, and all
patients with CRPS-related dystonia and hypothesized
patients used a baclofen solution of 3 mg/mL.
that the clinical efficacy may improve by increasing the IRwithout affecting safety as the daily dose was fixed.
In a double-blind, randomized, two-period, crossoverdesign, solutions of 3 and 0.75 mg/mL baclofen were
administered in a randomized sequence. A computermethod was used to randomly allocate patients to one of
The study was conducted in an ambulatory setting
the two sequences of different IRs. Prior to the start of the
between April and December 2008. Patient consent was
study, all patients received ITB at a simple continuous rate
obtained in accordance with the declaration of Helsinki,
with a 3 mg/mL concentration. To obtain two IRs at a 4:1
Intrathecal Baclofen Delivery in CRPS
ratio with a fixed daily dose, concentrations of 3 mg/mL
(slower infusion rate delivery [SIRD]) and 0.75 mg/mL(faster infusion rate delivery [FIRD]) were used. A physician
The results are expressed as median (interquartile range
who was not involved in the assessments of the patients
[IQR]). For all variables, a Wilcoxon signed rank test or
carried out the switch procedure at the start of each
Mann–Whitney U test was used to examine differences
sequence, filling the pump reservoir with baclofen concen-
within and between patients, respectively. A chi-square
trations of 0.75 or 3 mg/mL. Notably, reservoir fillings were
test was conducted to compare the amount of adverse
always changed, regardless of the assigned new concen-
events between the FIRD and the SIRD groups. Signifi-
tration to guarantee maintenance of blinding. When the
cance was assumed at the 0.05 level. Assuming an alpha
baclofen concentration is changed, a bridge bolus can be
of 0.05, beta of 0.2, a standard deviation of the NRS of 2,
used to empty the internal pump tubing and external
and a correlation between measures of 0.6, we calculated
catheter with the old baclofen concentration with the origi-
that 14 patients would be required to detect a statistically
nal IR. With a fixed daily administered dose, the replace-
significant difference of Ն25% in the reduction of NRS
ment of the 3 mg/mL concentration will result in a
substantial delay before the new concentration reachesthe tip of the catheter. As this concentration-dependent
delay may potentially contribute to deblinding, we usedthe side port to carry out a procedure that included aspi-
Demographic and Baseline Characteristics
ration of the content of the external catheter followed bymultiple boluses to replace the removed volume. As a
Fourteen CRPS patients (13 women) aged 45.5 years
result of this approach, the new concentration would
(IQR 37.3–56.0) with a median disease duration of 12.5
always reach the tip of the catheter within an hour regard-
years (IQR 8.0–16.3) were found eligible and participated
less of the old concentration. During the first 2 weeks of
in the study (Table 2). The median daily dose of ITB was
the study, the first assigned IR was used. This was fol-
695 mg (IQR 393–838), with the median thoracic level of
lowed by a 1-week open administration of the 3 mg/mL
the catheter tip at T7 (range T2–T11). Seven patients (six
concentration of baclofen to minimize potential conse-
women) were allocated to the FIRD–SIRD sequence;
quences of any carryover effect. Subsequently, over the
seven patients (all women) were allocated to the SIRD–
following 2 weeks, patients received the other IR.
FIRD sequence. All patients completed the study. A Wil-coxon signed rank test indicated there were no significant
Patients were asked to rate the global severity of pain and
dystonia using an NRS ranging from 0 (absent) to 10 (mostsevere) once every day starting 1 week before the first
switch procedure until the end of the second treatmentperiod. At the start and end of each treatment period prior
to changing the IR, a blinded clinical assessor rated the
dystonia severity using the Burke–Fahn–Marsden (BFM)
scale, which is the sum of the scores of the individual body
regions [20]. The same rater assessed the change of
CRPS signs and symptoms from baseline on a global
impression scale (GIS) at the end of each treatment,
ranging from -3 (much worse) to +3 (much better) with 0
for “no change.” At the end of the study, patients were
asked to compare both treatment periods using a patient
preference questionnaire (PPQ). The PPQ consists of a
10-cm horizontal line ranging from -5 to +5. A score of 0
reflects no preference, whereas -5 or +5 expresses
maximal preference for the first or second treatment
period, respectively. In addition, patients were asked to
indicate the reasons for their preference. At the end of
each study the clinical assessor was asked to guess treat-
ment assignment to evaluate the integrity of blinding. The
primary outcome measure was the difference in change in
global severity of pain and dystonia between baseline and
end of each IR period. The secondary outcome measures
were defined as the difference in change in BFM score
between baseline and end of each IR period, the differ-ence in GIS between both treatment periods, the PPQ
score, and the frequency and severity of adverse events
CRPS = complex regional pain syndrome; ITB = intrathecal
assessed at the end of each IR period. van der Plas et al.
Baseline scores for primary and secondary outcome measures
NS = not significant; FIRD = faster infusion rate delivery; SIRD = slower infusion rate delivery; NRS = numeric rating scale.
differences between baseline measures (NRS for dystonia
sion headache and likely resulted from aspiration of cath-
and pain and BFM) of the first and second treatment
eter content during the switch procedure. Two patients
period for each sequence, indicating a successful
reported one adverse event (both mild) while on SIRD
washout (Table 3). Additionally, a Mann–Whitney U test
including one patient with intracranial hypotension head-
indicated that there were no significant differences
ache. There were significantly more adverse events on
between these baseline measures of patients assigned to
FIRD compared with SIRD (c2 = 6.78, df = 1, P = 0.01),
each treatment sequence (FIRD–SIRD or SIRD–FIRD).
even after the removal of events due to intracranialhypotension (c2 = 6.97, df = 1, P = 0.01).
There were no significant differences between the FIRD
and the SIRD group in median change of NRS score fordystonia (–0.3 [IQR -1.1–0.5]) and pain (0.1 [IQR –0.8–
None of the demographics or clinical characteristics pre-
1.3]) and BFM score (2 [IQR -4–13]) (Table 4). Six patients
dicted any outcome measures except for the reason of
preferred FIRD with a median PPQ score of 3.0 (IQR
inclusion in the study, which was related to the preference
1.6–4.3), and seven patients favored the SIRD with a
median PPQ score of 3.0 (IQR 1.0–3.0). One patient hadno preference for any of the IRs. The difference between
Six out of eight patients, who entered the study because
both groups in PPQ score was not significant. After FIRD,
side effects prohibited dose escalation of ITB, reported
six patients showed an improvement on the GIS (+1 in four
preference for FIRD because dystonia and pain improved
and +2 in two patients), three patients deteriorated (–1 in
(median PPQ score 2.5 [IQR -1.4–3.8]). All six patients,
two and -2 in one patient), and five patients showed no
who entered the study because they did not respond to a
change. After SIRD, four patients showed an improvement
minimum daily dose of 600 mg ITB without baclofen-
on the GIS (+1 in three and +3 in one patient), three
related side effects, preferred SIRD, except one patient
patients deteriorated (–1 in one and -2 in two patients),
who reported no preference for any of the IRs (median
and seven patients showed no change. There was no
PPQ score 2.0 [IQR 0.8–3.5]). Mann–Whitney U test
significant difference in change found on the GIS score
revealed a significant difference in patient’s preference
between both IRs (z = –1.66). There was no significant
(P = 0.03) between groups, stratified according to “reason
effect of IR sequence on any of the outcome measures.
of participation.” No significant difference was found for
Twelve adverse events (five moderate, seven mild) were
any of the other primary and secondary outcomes as well
reported in eight patients on FIRD (Table 5). Headache
as the rate or severity of adverse events between both
was the most frequently reported adverse event (N = 5),
groups (P > 0.05). The clinical assessor’s guess of which
which in three patients was typical of intracranial hypoten-
IR was administered was correct in 57%.
Difference in change for primary and secondary outcome measures
Negative values represent improvement in outcome measures. P values were derived from a Wilcoxon signed rank test. NS = not significant; FIRD = faster infusion rate delivery; SIRD = slower infusion rate delivery; IQR = interquartile range;NRS = numeric rating scale. Intrathecal Baclofen Delivery in CRPS
implanted pump [16]. These poor responders includedpatients who failed to improve Ն25% in global dystonia
severity in spite of repeated dose escalations (up to600 mg/24 hours) and patients in whom dose escalation
was limited because of the occurrence of side effects. Interestingly, the intrathecal IR applied during the screen-
ing period exceeded the IR of the postimplantation period
as much as seven times because a lower concentration
(0.5 mg/mL) was used. Additionally, the daily dose at the
time patients qualified for the responder criterion of the
screening procedure was lower in the majority of patients
compared with the daily dose administered during the
postimplantation period (Table 1). Triggered by these find-ings, we evaluated if different IRs at a fixed daily dose
influence the efficacy and safety of ITB in patients with
SIRD = slower infusion rate delivery; FIRD = faster infusion rate
CRPS-related dystonia. In addition to dystonia, we evalu-
ated the influence of ITB on pain because baclofen mayexert an analgesic effect [22]. Prior to the start of this study
Discussion
none of the patients experienced a beneficial response inpain to ITB. Both for the total group as well as the sub-
Intrathecal drug delivery has opened new avenues for the
groups defined by reason of inclusion, we found no differ-
administration of drugs like baclofen that have difficulty
ences between FIRD and SIRD on any of the primary
passing the blood–brain barrier. However, once the drug is
outcome measures. Blinding was adequately maintained,
in the intrathecal space, many aspects may influence its
as the sequence of IRs was correctly guessed in approxi-
profile of efficacy and safety [21]. One of these aspects is
mately half of the cases. Our findings may indicate that IR
the IR of a drug, which surprisingly has barely been
differences up to a factor four do not account for the lack
explored [17,18]. In a recent study on long-term effects of
of response to ITB in implanted patients. Although we
ITB in CRPS-related dystonia, we noted that a substantial
cannot exclude that the difference between the two IRs
percentage of patients, who responded to ITB during a
was too small to detect a clinically relevant difference, the
screening procedure using an external pump, subse-
use of a four-times higher IR seemed appropriate. The use
quently failed to respond to continuous ITB with an
of a concentration below 0.75 mg/mL would have implied
Figure 1 Box plot illustrating patient’s preference for patients with a poor response with and without van der Plas et al.
an extra refilling of the pump during the FIRD period in
headache during FIRD and consequently preferred SIRD.
some patients, which may have caused deblinding. The
However, it deserves emphasis that the aforementioned
majority of patients displayed dystonia in all extremities
findings are the result of post hoc subgroup analyses and
reflecting the referral of more severely affected patients to
hence warrant further investigation in future studies.
our tertiary center. One could argue the severity of dysto-
During the FIRD, patients reported significantly more
nia may account for the lack of response to ITB. However,
adverse events of a supraspinal origin. As the daily dose of
only patients who had demonstrated responsiveness to
ITB was fixed for both IRs, this finding likely suggests a
ITB at an earlier stage were included in this study. Another
more extended intrathecal distribution of baclofen with
limitation of this study could be the large variability in the
daily administered dose of ITB across the patients, whichreflects individual differences with respect to the dose ofITB at which patients perceived some albeit insufficient
Conclusions
benefit (<25%) or the highest tolerated dose that did notcause unacceptable side effects. Consequently, it was not
In conclusion under a fixed daily dose, a four-times higher
possible to equalize the daily administered dose of ITB. On
IR enhances the intrathecal distribution of baclofen as
the other hand, using a crossover design, patients served
evident from the significantly higher number of adverse
as their own controls with the daily dose fixed for each
events. However, in CRPS a fourfold higher IR is not
patient. Contrary to the primary outcomes, patient’s pref-
associated with clinically overt improvement of dystonia or
erences indicated significant differences with respect to
pain. Patients in whom side effects restricted further dose
the preferred IR. Except for one case, all patients who
escalations of ITB favored FIRD because of subjective
were included because they failed to respond to sequen-
improvement of dystonia and pain. In these patients, FIRD
tial dose escalations of ITB (without baclofen-related side
did not cause more side effects than in patients who failed
effects) favored SIRD. Surprisingly, the majority of patients,
to respond to ITB after subsequent dose escalations but
who were included in the study because side effects
who had not experienced side effects. Consequently, in
restricted further dose escalation of ITB, reported a pref-
the subgroup of patients in whom side effects prevent ITB
erence for FIRD. In a written statement delineating their
dose escalation, the effect of increasing the IR of ITB at a
preference, all but one patient in both subgroups revealed
fixed daily dose should be further investigated.
that their preference was based on the influence of the IRon dystonia and pain, which apparently outweighed the
Disclosure of Funding
There was no funding or financial support received from
Of note is that patients’ preferences were paralleled
any funding agency, individual, organization, or other kind
neither by changes in primary and secondary outcome
measures of dystonia nor by the clinical impression ofchange, which may question the responsiveness of theapplied assessment scales to subtle changes. Possibly,
Conflicts of Interest
increasing the IR under a fixed daily dose reduces theseverity of side effects as compared with increasing the IR
All authors report no financial interest on the subject
by raising the daily dose. In 11 patients, a screening
matter or any competing materials. Sam Eldabe currently
procedure was performed prior to pump implantation.
receives research funding from Medtronic and has also
Interestingly, patients who participated in the study
received honoraria for lectures given on Medtronic’s
because ITB-related side effects limited dose escalation
behalf in the last year. Eric Buchser’s employer, EHC
had a significantly larger difference between the IRs of the
Hospital of Morges, has received research and educa-
screening and postimplantation, compared with patients
tional grants from Medtronic sàrl, Tolochenaz Switzerland.
with a poor response without side effects (Table 6). All
Jacobus Johannes van Hilten has been a consultant for
patients of the first category favored FIRD, except for one
Medtronic and has received an unconditional research
patient, who suffered from severe intracranial hypotension
Ratios of drug delivery characteristics for screening vs postimplantation period
The screening to postimplantation period ratio for infusion rate and daily dose for patients with a poor response with and without sideeffects to intrathecal baclofen [16]. P values were derived from a Mann–Whitney U test. IQR = interquartile range. Intrathecal Baclofen Delivery in CRPS References
optimal therapeutic responses in spastic paresis. J
1 Veldman PH, Reynen HM, Arntz IE, Goris RJ. Signs
and symptoms of reflex sympathetic dystrophy:Prospective study of 829 patients. Lancet 1993;
13 Leisen C, Langguth P, Herbert B, et al. Lipophilicities
of baclofen ester prodrugs correlate with affinities tothe ATP-dependent efflux pump P-glycoprotein: Rel-
2 Merskey H, Bogduk N, eds. Classification of Chronic
evance for their permeation across the blood-brain
Pain. Description of Chronic Pain Syndromes and Defi-
barrier. Pharm Res 2003;20(5):772–8.
nition of Pain Terms, 2nd edition. Seattle, WA: IASPPress; 1994:40–3.
14 Jones RF, Anthony M, Torda TA, Poulos C. Epidural
baclofen for intractable spasticity. Lancet 1988;
3 Janig W, Baron R. Complex regional pain syndrome:
Mystery explained. Lancet Neurol 2003;2(11):687–97.
15 van Hilten BJ, van de Beek WJ, Hoff JI, Voormolen JH,
4 Schwartzman RJ, Kerrigan J. The movement disorder
Delhaas EM. Intrathecal baclofen for the treatment of
of reflex sympathetic dystrophy. Neurology 1990;
dystonia in patients with reflex sympathetic dystrophy.
5 Harden RN, Bruehl S, Galer BS, et al. Complex
regional pain syndrome: Are the IASP diagnostic cri-
16 van Rijn MA, Munts AG, Marinus J, et al. Intrathecal
teria valid and sufficiently comprehensive? Pain
baclofen for dystonia of complex regional pain syn-
6 van Rijn MA, Marinus J, Putter H, van Hilten JJ. Onset
17 Bernards CM. Cerebrospinal fluid and spinal cord dis-
and progression of dystonia in complex regional pain
tribution of baclofen and bupivacaine during slow
syndrome. Pain 2007;130(3):287–93.
intrathecal infusion in pigs. Anesthesiology 2006;105(1):169–78.
7 Fahn S, Bressman SB, Marsden CD. Classification of
dystonia. Adv Neurol 1998;78:1–10.
18 Buchser E, Durrer A, Chedel D, Mustaki JP. Efficacy of
intrathecal bupivacaine: How important is the flow
8 Bhatia KP, Bhatt MH, Marsden CD. The causalgia-
dystonia syndrome. Brain 1993;116(Pt 4):843–51.
19 Munts AG, van der Plas AA, Voormolen JH, et al.
9 van de Beek WJ, Vein A, Hilgevoord AA, van Dijk JG,
Intrathecal glycine for pain and dystonia in complex
van Hilten BJ. Neurophysiologic aspects of patients
regional pain syndrome. Pain 2009;146(1–2):199–
with generalized or multifocal tonic dystonia of reflex
sympathetic dystrophy. J Clin Neurophysiol 2002;19(1):77–83.
20 Burke RE, Fahn S, Marsden CD, et al. Validity and
reliability of a rating scale for the primary torsion dys-
10 Malcangio M, Bowery NG. GABA and its receptors in
tonias. Neurology 1985;35(1):73–7.
the spinal cord. Trends Pharmacol Sci 1996;17(12):457–62.
21 Bennett G, Serafini M, Burchiel K, et al. Evidence-
11 Orsnes G, Crone C, Krarup C, Petersen N, Nielsen J.
based review of the literature on intrathecal delivery of
The effect of baclofen on the transmission in spinal
pain medication. J Pain Symptom Manage 2000;
pathways in spastic multiple sclerosis patients. Clin
22 Zuniga RE, Schlicht CR, Abram SE. Intrathecal
12 Knutsson E, Lindblom U, Martensson A. Plasma and
baclofen is analgesic in patients with chronic pain.
cerebrospinal fluid levels of baclofen (Lioresal) at
Press Release Contact: Emily Esterson MFHA/Covertside 505-553-2671 [email protected] Masters of Foxhounds Association to Offer Thoroughbred Incentive Awards in 2013 Berryville, Va.—The Masters of Foxhounds Association (MFHA) is proud to announce that 2013 is The Year of the Foxhunting Thoroughbred. The MFHA is offering $750 in cash and prizes to a hunt member and a hunt club
PETER HESSELDAHL GROUND RULES FOR THE 21ST CENTURY Chapter 14 THERE MUST BE ROOM FOR ERROR You probably remember being a child, studying a ladybug crawling up a leaf of grass, upwards towards the sunlight. Eventually, it reaches the tip, where it can’t climb any further – so it spreads its wings and flies. But what do you do if you don’t have wings? There are two possibilities: E
 Pain Medicine 2011; 12: 459–465Wiley Periodicals, Inc.
NEUROPATHIC PAIN SECTION
Pain Medicine 2011; 12: 459–465Wiley Periodicals, Inc.
NEUROPATHIC PAIN SECTION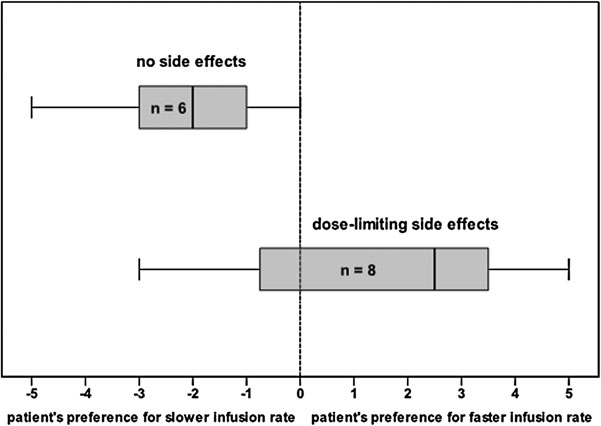 Intrathecal Baclofen Delivery in CRPS
Intrathecal Baclofen Delivery in CRPS