La spécificité du tadalafil est liée à sa longue demi-vie, permettant une action qui excède largement celle des autres inhibiteurs de PDE5. L’absorption digestive est complète, avec un pic plasmatique atteint en 2 heures environ. Le métabolisme est réalisé via CYP3A4, produisant des métabolites inactifs éliminés principalement dans les fèces. La sélectivité enzymatique est élevée, réduisant les effets indésirables extra-caverneux. Les réactions indésirables fréquentes incluent céphalées, bouffées vasomotrices et troubles digestifs légers. L’activité pharmacologique est stable, indépendamment de l’ingestion d’aliments. Dans les comparaisons de longue durée, acheter cialis pas cher est mentionné en relation avec les études portant sur la persistance d’efficacité et la constance de la cinétique plasmatique.
Comepa.com.uy
Evolution of Antimicrobial Resistance:Impact on Antibiotic Use
Didier Guillemot, M.D.,1 Anne Claude Crémieux, M.D.,2 and Patrice Courvalin, M.D.1 ABSTRACT
During the past 50 years, the permanent increase in bacterial resistance to antibi-
otics has led to modifications in therapeutic recommendations. Despite evidence that an-timicrobial exposure of human populations is the most important driving force for thecontinuous increase in bacterial resistance, the studies of the impact of bacterial resistanceon antibiotic use have, during the past, focused on clinical efficacy of individual treatmentsrather than on collective control of resistance. There are current changes in this attitude,mainly in hospitals, probably because hospital prescribers have experienced the conse-quences of resistance on their patients. However, in the community such an awareness isnot likely to develop in the near future. Therefore, there is a need for public health decisionmakers to become more involved in prevention of the impact of resistance in antibiotic use. KEYWORDS: Antimicrobial resistance, antibiotic use, therapeutic decision, drug policy Objectives: Upon completion of this article, the reader will be able to: (1) describe the problem of treating community and nosoco- mial infections in the face of increasing prevalence of resistant pathogens; and (2) define collective strategies for maintaining an- timicrobial efficacy in the hospital and in the community. Accreditation: The University of Michigan is accredited by the Accreditation Council for Continuing Medical Education to sponsor continuing medical education for physicians. Credits: The University of Michigan designates this educational activity for a maximum of 1.0 hour in category one credits toward the AMA Physicians Recognition Award.
Antimicrobial resistance has emerged as a major ceptible organisms.4 Repeated warnings have been is-
public health concern worldwide. During the past
sued on the development of bacterial resistance to an-
decades, despite the continuous marketing of new an-
tibiotics and the related threats to the effectiveness of
tibiotics, antimicrobial resistance has increased steadily.
available antibiotics. Many researchers have predicted
In hospitals, roughly 70% of bacterial pathogens are re-
doom and gloom scenarios, claiming that a considerable
sistant to at least one antibiotic.1 Patients with infec-
proportion of infections will become steadily more dif-
tions due to resistant organisms are likely to require more
and longer hospital stays,2 and to die.3 Furthermore, the
Although estimation of risks associated with the
collective economic cost of infections with resistant bac-
use of antibiotics based on a single bacterium–resistance
teria seems to be much higher than for those with sus-
mechanism model cannot be strictly extrapolated to an-
Hospital-Acquired Pneumonia; Editor in Chief, Joseph P. Lynch, III, M.D.; Guest Editor, Mark J. Rumbak, M.D. Seminars in Respiratory andCritical Care Medicine, volume 23, number 5, 2002. Address for correspondence and reprint requests: Patrice Courvalin, M.D., Unité des AgentsAntibactériens–Centre National de Reference des Antibiotiques, Institut Pasteur, 25–28 rue du Dr. Roux, 75724 Paris Cedex 15. Email:[email protected]. 1Unité des Agents Antibactériens–Centre National de Reference des Antibiotiques, Institut Pasteur, Paris, France; 2HopitalBichat–Faculté de Médecine Bichat Claude Bernard, Paris, France. Copyright 2002 by Thieme Medical Publishers, Inc., 333 Seventh Avenue,New York, NY 10001, USA. Tel: +1(212) 584-4662. 1069-3424,p;2002,23,05,449,456,ftx,en;srm00174x. SEMINARS IN RESPIRATORY AND CRITICAL CARE MEDICINE/VOLUME 23, NUMBER 5 2002
other pair, the causal relationship between exposure of
classes of drugs that are not related structurally and dif-
human populations to antibiotics and the progression of
bacterial resistance to the same molecules should be
Co-resistance is due to the presence in the same
considered an established fact. Numerous studies have
bacterium of several mechanisms, each conferring resis-
demonstrated this association in both the hospital6 and
tance to an antibiotic class. The corresponding genes are
often part of the same replicon (chromosome or plas-
Thus, there are two main reasons for optimizing
mid), which results in co-dissemination—vertically to
antibiotic use: (1) the increased recognition of inadequate
the progeny if the resistance determinants are located in
antimicrobial treatment both in the community and in
the chromosome; both vertically and horizontally by
hospital settings and its potential impact on the outcome
lateral gene transfer for genes located on self-transfer-
of severe infections (individual approach), and (2) evi-
able plasmids or conjugative transposons. In the case of
dence and general consensus in the medical community
S. pneumoniae the multidrug-resistant (to penicillins,
that resistance to antimicrobial drugs is clearly linked to
macrolides, tetracycline, chloramphenicol, trimethoprim,
the consumption of antibiotics (collective approach).
and sulfonamides) strains have the resistance genes sta-
For the past 50 years, evolution of resistance has
bilized in their chromosome. Because dissemination of
led to modifications in the use of antibiotics, but there is
pneumococci is clonal, a few distinct bacteria account
no evidence that these modifications, even the more re-
for a worldwide evolution of this species toward mul-
cent ones, have combined optimization in clinical effi-
cacy (individual approach) and delay in the progression
In gram-negative bacteria, such as Klebsiella
of antimicrobial resistance in human pathogens. pneumoniae, P. aeruginosa, and Acinetobacter spp., a veryelegant system of gene capture and expression, namedintegron, is responsible for co-resistance to multipledrug classes.14,15 The net result of these genetic elements
HOW ANTIBIOTIC USE SHOULD BE
is to assemble and express in a coordinated fashion a
INFLUENCED BY RESISTANCE
large collection of genes, each conferring resistance to a
MECHANISMS
Resistance of bacteria to antibiotics can result from a vari-
As far as therapy is concerned, the most impor-
ety of phenomena. There are various biochemical mecha-
tant consequence is that cross-resistance means cross-
nisms (detoxification of the drug, alteration of the target
selection and co-resistance means co-selection. In other
of the drug, impermeability of the bacteria to the antibi-
words, the use of any antimicrobial to which the strain is
otic8 or bypass, different genetic bases (chromosome, plas-
resistant will favor dissemination of resistance not only
mids, transposons9 and various ways of emergence (muta-
to itself and to the other members of the same class
tional event, acquisition of foreign genetic information9 of
(cross-resistance) but also to various classes of drugs (in
resistance. In addition, these bacterial approaches to resis-
case of extended cross-resistance or co-resistance) that
tance are not mutually exclusive and often coexist in the
are structurally unrelated to the antibiotic that exerts the
same prokaryotic host often leading to multiresistance.10
selective pressure. This has obvious implications on the
We will consider certain aspects of resistance that are
“cycling” of antibiotics, which consists of the rotation of
common in bacteria responsible for respiratory diseases
drugs in a given ecosystem (ward, hospital, community).
and that should be, ideally, kept in mind prior to therapy.
There are pitfalls in the detection of resistance
Bacteria can become multiresistant in two ways:
phenotypes that can be expressed at low levels. For ex-
cross-resistance or co-resistance. In the phenomenon of
ample, resistance can be inducible, (i.e., expressed only
cross-resistance, a single biochemical mechanism is re-
when the bacterium is in the presence of sub-inhibitory
sponsible for resistance of the host bacterium to various
concentrations of the inducing antibiotic in the envi-
levels of all the members of a class of antibiotics. For ex-
ronment).9 Because induction can be a slow process,
ample, resistance to fluoroquinolones in Streptococcus
rapid techniques of determination of in vitro suscepti-
pneumoniae can be secondary to mutations in the targets
bility may fail to detect this type of resistance, such as
of the drugs, the type II topoisomerases.9 However,
glycopeptide resistance in enterococci.16 Alternatively
cross-resistance to various antibiotic classes can also be
certain mechanisms, in particular efflux, often confer
due to a single mechanism, for example drug efflux. The
low-level resistance that could have clinical consequences.
substrate specificity of the pumps that export antibiotics
Selection of resistant mutants can occur under
can be very large and, for example, confer in Pseudomo-
therapy. Although macrolides, lincosamides, and strep-
nas aeruginosa decreased susceptibility to -lactams,
togramins (MLS) are chemically unrelated, a specific
aminoglycosides, tetracyclines, chloramphenicol, trimeth-
modification in the ribosome can confer high-level re-
ropim, sulfonamides, fluoroquinolones, and macrolides,
sistance to the three classes of antibiotics. This resis-
lincosamides, and streptogramins.11,12 This leads to the
tance phenotype, which is due to the fact that the vari-
notion of extended cross-resistance (i.e., resistance to
ous drugs have overlapping targets on the ribosome, is
EVOLUTION OF ANTIMICROBIAL RESISTANCE/GUILLEMOT ET AL
inducible by low concentrations of 14-member (ery-
main active as penicillinases but have evolved to become
thromycin, roxithromycin, clarithromycin, and often
also cephalosporinases (conferring resistance to all ceph-
oleandomycin) and 15-member (azithromycin) only, the
alosporins but cephamycins, cefoxitin, and cefotetan) or
other antibiotics remaining active. However, MLS that
resistant to inhibitors of penicillinases (clavulanic acid,
are noninducers can select only one-step regulatory mu-
sublactam, and tazobactam). Because the structural genes
tants that are cross-resistant to the three drug classes, as
for the enzymes are most often located on plasmids that
has been reported in Staphylococcus spp. and in other
are self-transferable by conjugation, the emergence and
spread of these enzymes represent an interesting exam-
As already mentioned, quinolones act by binding
ple of cross-resistance to nearly all -lactams by what
to type II topoisomerases, DNA gyrase, and topoiso-
could be considered as “infectious mutations.”
merase IV, and S. pneumoniae can become resistant by
Acinetobacter spp. are opportunistic pathogens
alteration of the target but also by efflux of the drugs. In
that often colonize and infect patients in intensive care
both cases, resistance is secondary to a mutational event:
units. Acinetobacter baumannii has been found to be re-
a regulatory mutation leading to overexpression of an
sponsible for epidemic nosocomial pneumonia, and few
efflux pump or a mutation in a structural gene resulting
drugs are active because of the number of resistance
in a decrease in the affinity of the target for the drugs.18
mechanisms accumulated by the bacteria.23 The high
The higher the number of mutations, the higher the
rate of treatment failures and deaths caused by Acineto-
levels of resistance, and the higher the intrinsic activity
bacter infections suggests that for certain bacterial
of the drug, the lower the level of resistance. However,
pathogens, better be resistant than virulent.
and again in this class of antibiotics, there is clearlycross-resistance between all the drugs belonging to theclass.9
For both MLS and fluoroquinolones, the emer-
IMPACT OF RESISTANCE ON
gence of resistance under therapy, although it has been
CLINICAL RECOMMENDATIONS
documented, does not represent the major threat. As al-
(THE INDIVIDUAL APPROACH)
ready discussed, dissemination of antibiotic resistance in
Antimicrobial resistance has clearly stressed the need to
S. pneumoniae, like in Staphylococcus aureus, is clonal; in
optimize antibiotic therapy in community and hospital
other words, a few epidemiologically successful multire-
settings. In the community, regardless of whether we are
sistant clones have, for yet unknown reasons, dissemi-
dealing with bacteria responsible for respiratory, urinary,
nated worldwide. Thus the spread of resistance to MLS
or sexually transmitted infections, evolution toward re-
or fluoroquinolones or, even worse, to both, will be sec-
sistance is progressively accompanied by modifications
ondary to colonization of patients by already resistant
in the therapeutic recommendations for first-line an-
clones. This also holds true for strains of enterococci
tibiotic therapy. In response to the increased number of
and staphylococci that are beginning to become resis-
Haemophilus influenzae strains producing -lactamases,
tant to the new class of drugs, the oxazilidinones.19,20
guidelines for the treatment of otitis have favored a
Repeated cures of antibiotics can lead to the se-
combination of aminopenicillin and a -lactamase in-
lection of hypermutator strains, in particular of P. aerug-
hibitor.24–27 Furthermore, the appearance and, above all,
inosa21 and S. aureus in patients suffering from cystic fi-
the wide dissemination of penicillinase-producing S.
brosis (R. Leclercq, personal communication, 2001). aureus strains has led to the conclusion that community
Bacteria with elevated (up to 1000-fold) mutation rates
acquired S. aureus infections can no longer be treated
have in certain ecosystems a clear advantage to adapt to
the repeated sudden and strong selective pressure ex-
Among community acquired pathogens, resistance
erted against them by antibiotic therapy. S. aureus clini-
to antibiotics has increased.28 However, some commonly
cal isolates that are resistant to methicillin, and thus to
used antibiotics remain effective. The most worrisome
all -lactams, are nearly always resistant to fluoroquino-
problem is S. pneumoniae resistance because this species
lones. The latter class of drugs is increasingly used, in
is the main cause of potentially life-threatening commu-
particular for pulmonary infections. One could therefore
nity acquired diseases such as meningitis and pneumo-
anticipate that because of co-resistance to the two
nia. In meningitis, delayed administration of appropriate
groups of antibiotics and clonal dissemination of staphy-
therapy has been linked to poor outcome.29 Retrospec-
lococci, massive use of fluoroquinolones will select for
tive studies on pneumococcal meningitis in children30 or
strains resistant to both -lactams and fluoroquinolones,
in intensive care units31 failed to show that nonsuscepti-
in particular in community-acquired infections.
bility to penicillins was associated with a worse outcome.
Extended spectrum -lactamases are predomi-
Decreased pneumococcal susceptibility to penicillin G has
nantly found in K. pneumoniae, an enterobacterial species
led to recommendations to increase the doses of amino-
responsible for pulmonary infections. The enzymes are
penicillin.32 Nevertheless, use of third generation ceph-
point mutants of “old” penicillinases.22 The proteins re-
alosporins has been shown to lead to treatment failure in
SEMINARS IN RESPIRATORY AND CRITICAL CARE MEDICINE/VOLUME 23, NUMBER 5 2002
meningitis caused by S. pneumoniae with MIC ≥ 0.5
into account the pharmacokinetic parameters of the
µg/mL.29 For pneumococcal meningitis, increased resis-
tance to -lactams has resulted in the recommendation
As an example of the latter statement, bacteria
of an injectable third-generation cephalosporin (cefo-
responsible for infection can be initially susceptible to
taxime or ceftriaxone) first-line prescription33 in combi-
the antibiotic administered and become resistant during
nation with a glycopeptide (vancomycin).34 However, one
therapy. In nosocomial infections due to P. aeruginosa
can anticipate that if the level of resistance to penicillins
susceptible to ciprofloxacin, it has been shown that an
continues to rise, it could render -lactams even in com-
AUC :MIC ratio ≤ 110 can be significantly associated
bination with glycopeptides increasingly less effective,
with the emergence of ciprofloxacin resistance.40 Thus,
resulting in deterioration of the prognosis of pneumo-
high dosages of fluoroquinolones have been recommended
coccal meningitis by delay in active therapy. This under-
to avoid resistance in P. aeruginosa infection. Doses assur-
lines the need to continue to update recommendations
ing tissue concentrations well above the mutant selection
window are, along with drug combinations, strategies used
The situation is very different in the field of hos-
to restrict development of resistance during therapy.
pital-acquired infections. In many circumstances, only
To date, even though the impact of antibiotic
very few antimicrobial agents remain effective in partic-
treatment on the commensal flora has been widely doc-
ular against methicillin-resistant S. aureus or multidrug
umented41 how that impact can influence on individual
resistant gram-negative bacteria. Although several stud-
therapeutic remains currently questionable.
ies have failed to show that nosocomial infections due toantibiotic-resistant bacteria are associated with higherattributable mortality rates than infections caused by
IMPACT OF RESISTANCE ON ANTIBIOTIC
their susceptible counterparts, other studies have shown
USE POLICIES (THE COLLECTIVE
that administration of inadequate initial antimicrobial
APPROACH)
therapy is associated with adverse outcome in critically
The impact of bacterial resistance on selection of the
ill patients35,36 or after intraabdominal surgery.35,37 In
antibiotics to be used may also be analyzed from a pub-
these studies the poorer outcome was mainly related to
lic health point of view. This automatically raises the
inadequate initial antimicrobial therapy due to antibi-
question of the existence of a collective regulatory
otic-resistant gram-positive or -negative bacteria. Fur-
mechanism between the progression of this resistance in
thermore, prior antibiotic use or prior use of broad spec-
bacteria responsible for infections and the prescription
trum antibiotics have been shown to be associated with
of antibiotics. In other words, the problem is to deter-
ventilator-associated pneumonia caused by antibiotic
mine whether the continued expansion of bacterial re-
sistance could spontaneously lead to a modification in
In bone and joint infections however, methicillin-
antibiotic prescription practices and, if so, whether this
resistant S. aureus (MRSA) could have a significant im-
change itself can, in turn, have an impact on resistance.
pact on the management or the outcome of infections.
As discussed above, the progression of resistance in
Direct exchange arthroplasty is not recommended in in-
pathogenic bacteria to commercialized antibiotics has
fections due to MRSA because of a significant number
regularly led to the modification of therapeutic recom-
of failures.38 In poststernotomy mediastinitis, MRSA
mendations, both in hospitals and in the community.
has been observed as the only independent risk factor
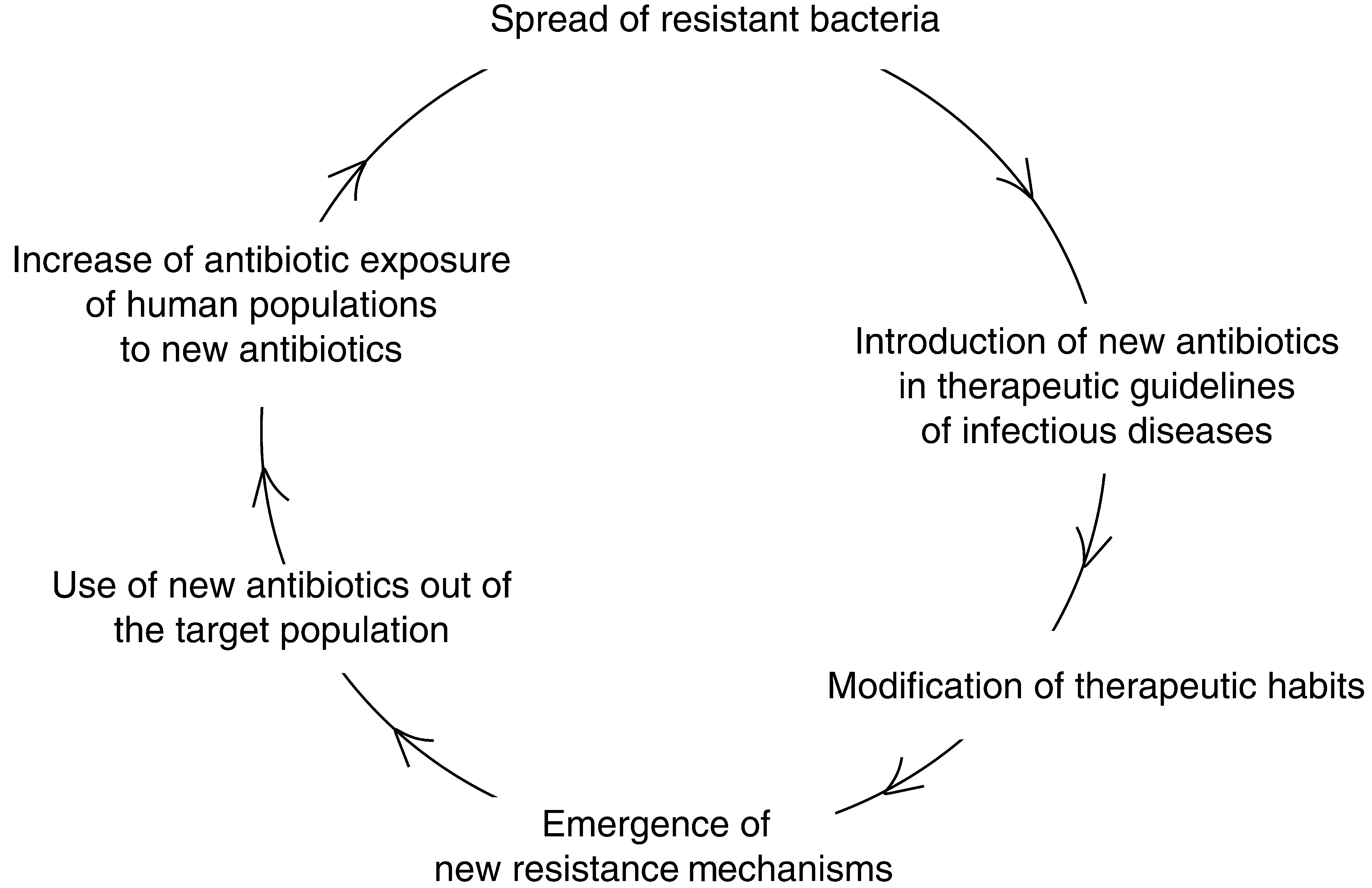
The evolution of treatment guidelines has pri-
for overall mortality.39 Glycopeptides, in monotherapy
marily and naturally been characterized by the preoccu-
or in combination, are used as first-line therapy for
pation with encouraging the prescription of antibiotics
prosthethic and poststernotomy infections because the
to which the bacteria are still susceptible; that is to say,
vast majority of MRSA remains sensitive to these an-
the use of ever more recent molecules. Emergence and
tibiotics. Even though glycopeptides remain the refer-
spread of resistance to newer antibiotics is the result of
ence therapy for MRSA infection, these drugs may not
this approach as illustrated by what has been observed
be optimal because they are slowly bactericidal. Thus,
the poorer prognosis of MRSA infection could reflect
This evolution is logical because the basic goal of
the long time it takes the molecule to diffuse in bone.
the prescriber is to preserve the individual’s clinical ben-
Taken together, these observations underline the
efit of the therapeutic intervention. Encouraging changes
need (1) to avoid unnecessary use of antimicrobials, es-
in antibiotic use with the objective of mastering bacter-
pecially broad spectrum antibiotics in hospitalized pa-
ial resistance presupposes (1) decreasing the amount of
tients, (2) to establish local guidelines taking into ac-
prescribed antibiotics by restricting their use to true
count local epidemiology and resistance patterns, (3) to
bacterial infections, (2) optimizing their use based on
develop rapid tests to detect resistance in order to opti-
their pharmacokinetic and pharmacodynamic charac-
mize the efficacy of the initial therapy and spare the use
teristics, (i.e., by adapting dose and duration), (3) avoid-
of broad spectrum antibiotics, and (4) to accurately take
ing unuseful antibiotic administration. EVOLUTION OF ANTIMICROBIAL RESISTANCE/GUILLEMOT ET AL Figure 1 The logic of maximizing only clinical efficacy. The Physician Level
timicrobial resistance requires both infection control
At the hospital setting, use of antibiotics has been
measures and regulation of antibiotic use and that either
shown to be one of the main risk factors for coloniza-
alone is insufficient.72 This leads to close collaboration
tion by resistant bacteria and thus for infections due to
among the disciplines of infectious diseases, microbiol-
resistant organisms.42 Therefore, it is essential to dimin-
ogy, hospital epidemiology, pharmacy, and nursing with
ish these potential risk factors. Several studies covering
strong support from hospital leadership. One can expect
antibiotic policies at the hospital have shown that re-
that such a dynamic will soon result in an effective pro-
stricting the use of antimicrobials can alter prescribers’
gram that can be readily incorporated into the quality-
behavior.43–48 These studies also suggest that such a pol-
improvement goals of any health care organization.72
icy can have an impact on bacterial resistance.45,49–53
In the community and in many countries, viral res-
Strategies aimed at optimizing antibiotic prescription
piratory infections represent the main cause for prescrib-
are generally based on the use of order forms,54 of guide-
ing antibiotics73,74 and medical and scientific leaders have
lines, feedback to prescribers or next-day review of
voiced their concern that antibiotics are not justified in
antibiotic appropriateness,55,56 automatic stop-order 72
this clinical context. Several epidemiological studies have
hours after empiric prescription, rotating or combina-
shown that it is possible to reduce antibiotic prescription
tion therapies,57–60 and computer-based order entry.61–68
in the community.49,75,76 However, in countries with high
Thus, restricting the use of antimicrobial agents, pro-
community use of antibiotics, there is no evidence of any
viding locally adapted guidelines for the prudent use of
significant decline in the amount of these drugs, and
antibiotics, and implementing quality control of antimi-
countries in which antibiotics are not widely prescribed
crobial therapy within a hospital, in particular within
have generally been low antibiotic users in the past.
the intensive care unit, might help to minimize the se-
Thus, the question, Why do general practitioners
lection of multidrug-resistant bacteria.69 A recent study
overprescribe antibiotics? remains relevant. The most often
demonstrated that preapproval of selected parenteral
cited reasons for the “resistance” of prescribers to decrease
agents reduced the rates of antimicrobial-resistant
their use of antibiotics are the expectations of patients;
pathogens without compromising patients’ outcome.46
physicians often cite parents’ and patients’ pressure as fac-
Monitoring programs based on such axes are currently
tors in their decisions to prescribe antibiotics for viral
spreading in hospitals.70 Hospital health care workers
upper respiratory tract infections.77,78 Although physicians
are particulary concerned by bacterial resistance.71 They
are sometimes unable to evaluate patients’ expectations ac-
daily experiment bacterial resistance as a consequence of
curately,78 this may be one of the factors that limits the de-
inappropriate use of antibiotics. Therefore, such hospi-
crease of antibiotic use in the community, especially in
tal mobilization may result from the concern of hospital
urban areas where greater numbers of physicians must
physicians to both maximize the individual efficacy of
compete for patients. Another factor could be related to
their antibiotic prescriptions and minime the collective
the physician’s perception of bacterial resistance. Although
spead of bacterial resistance. Hospital physicians are be-
bacterial resistance to antibiotics is an iatrogenic drug
coming convinced that addressing the problem of an-
problem, the consequences are not yet obvious to the pre-
SEMINARS IN RESPIRATORY AND CRITICAL CARE MEDICINE/VOLUME 23, NUMBER 5 2002
scribers. It is unlikely that private practitioners can associ-
an impact on chronic morbidity and even mortality. As
ate their antibiotic prescriptions with infectious complica-
previously discussed, this necessitates decreases in the
tions in their patients that are due to bacterial resistance
exposure to antibiotics and the amounts of prescrip-
arising in their patients.Therapeutic failures attributable to
tions, which is to say, the volumes sold. At the same
bacterial resistance probably remain too uncommon to be
time, maximal clinical efficacy must be guaranteed; the
perceived by prescribers. In addition, selection of resistant
collective therapeutic efficacy of the management of
bacteria within the pharyngeal, digestive, or cutaneous
bacterial pathologies should not diminish. These objec-
flora constitutes the most potent mechanism leading to the
tives should probably take into consideration two con-
progression of resistance, but this is not tangible to the
straints: (1) in developed countries, the guarantee of
physician nor to the patient. In the community, physicians
minimal public health safety is the responsibility of the
do not appear to be concerned by bacterial resistance. The
national government, and (2) the sales pressure exerted
combined effect of patients’ pressure, lack of perception of
by the pharmaceutical industry constitutes a potent force
bacterial resistance, and the powerful image of the “new”
to increase the volume of drugs used.79 Henceforth, one
antibiotics may lead prescribers to use them outside the
of the solutions could be that negotiations between the
realm of strict recommendations. For example, the “broad
pharmaceutical industry, health care providers, and
spectrum” qualification, which has been widely used for the
the health insurance industry take into consideration
most-prescribed -lactams in the community, may have
the public health dimension of the potential consequences
contributed to an excess in their use outside the target pop-
ulation, thus to an increase in human exposure to antibi-otics and the resulting spread of new resistance mecha-nisms (Fig. 2). Henceforth, new solutions are needed. CONCLUSION Despite evidence that antimicrobial exposure of the human population is the most important factor for the The Level of Public Health Organization
permanent increase in bacterial resistance, the impact of
If the progression of bacterial resistance is not con-
the latter on antibiotic use has during the past focused
trolled, there is a short- or middle-term risk for an in-
mainly on clinical efficacy of individual treatment rather
crease in therapeutic failures, both in community ac-
than on collective control of resistance. It is striking to
quired infections such as bacterial otitis in children,
note the paradox between the driving force of the evolu-
sexually transmitted diseases, or urinary tract infections
tion of bacterial resistance and the main modifications
and in nosocomial infections. This rise will probably have
of precription practices. This underlies the difficulties
Figure 2 The example of evolution of Staphylococcus aureus toward multiresistance to antibiotics. EVOLUTION OF ANTIMICROBIAL RESISTANCE/GUILLEMOT ET AL
for practitioners to take into account the public health
22. Sougakoff W, Goussard S, Gerbaud G, Courvalin P. Plasmid-
mediated resistance to third-generation cephalosporins causedby point-mutations in TEM-type penicillinase genes. Rev In-fect Dis 1988;10:879–884
23. Bergogne-Bérézin E, Towner KJ. Acinetobacter spp. as noso-
REFERENCES
comial pathogens: microbiological, clinical, and epidemiolog-ical features. Clin Microbiol Rev 1996;9:148–165
1. Bruning LM. Emerging infectious diseases: threats to the
24. Magit AE, Stool SE. Clinical guideline development for oti-
OR? Interview by Kimberly Howell. Todays Surg Nurse
tis media: a report on methodology. Otolaryngol Head Neck
2. The cost of antibiotic resistance: effect of resistance among
25. Managing otitis media with effusion in young children. Staphylococcus aureus, Klebsiella pneumoniae, Acinetobacter bau-
American Academy of Pediatrics, The Otitis Media Guide-
mannii, and Pseudomonas aeruginosa on length of hospital stay.
Infect Control Hosp Epidemiol 2002;23:106–108
26. Managing otitis media with effusion in young children. Otitis
3. Carmeli Y, Troillet N, Karchmer AW, Samore MH. Health
Media Guideline Panel. Am Fam Physician 1994;50:1003–
and economic outcomes of antibiotic resistance in Pseudomo-nas aeruginosa. Arch Intern Med 1999;159:1127–1132
27. Otitis media with effusion in young children: guideline
4. Phelps CE. Bug/drug resistance: sometimes less is more. Med
overview. Agency for Health Care Policy and Research,
Rockville, Maryland. J Natl Med Assoc 1994;86:731–732,
5. Neu HC. The crisis in antibiotic resistance. Science 1992;
28. Goossens H, Sprenger MJ. Community acquired infections
6. Greenwood D. Preserving the miracle of antibiotics. Lancet
and bacterial resistance. BMJ 1998;317:654–657
29. Lebel MH, McCracken GH Jr. Delayed cerebrospinal fluid
7. Lipsitch M. Measuring and interpreting associations between
sterilization and adverse outcome of bacterial meningitis in
antibiotic use and penicillin resistance in Streptococcus pneu-
infants and children. Pediatrics 1989;83:161–167
moniae. Clin Infect Dis 2001;32:1044–1054
30. Buckingham SC, McCullers JA, Lujan-Zilbermann J, Knapp
8. Quintiliani R Jr, Sahm D, Courvalin P. Mechanisms of resis-
KM, Orman KL, English BK. Pneumococcal meningitis in
tance to antimicrobial agents. In: Murray PR, Jo Baron E,
children: relationship of antibiotic resistance to clinical charac-
Pfaller MA, Tenover FC, Yolken RH, eds. Manual of Clinical
teristics and outcomes. Pediatr Infect Dis J 2001;20:837–843
Microbiology. 7th ed. Washington, DC: American Society
31. Auburtin M, Porcher R, Bruneel F, et al. Pneumococcal
meningitis in the intensive care unit: prognostic factors of
9. Courvalin P, Trieu-Cuot P. Minimizing potential resistance:
clinical outcome in a series of 80 cases. Am J Respir Crit Care
the molecular view. Clin Infect Dis 2001;33(suppl 3):S138–
32. Guillemot D, Carbon C, Balkau B, et al. Low dosage and
10. Courvalin P. Combinatorial approach of bacteria to antibiotic
long treatment duration of beta-lactam: risk factors for car-
resistance. Res Microbiol 1999;150:367–373
riage of penicillin-resistant Streptococcus pneumoniae. JAMA
11. Paulsen IT, Brown MH, Skurray RA. Proton-dependent mul-
tidrug efflux systems. FEMS Microbiol. Rev 1996;60:575–608
33. Tan TQ, Schutze GE, Mason EO Jr, Kaplan SL. Antibiotic
12. Nikaido H. Multidrug efflux pumps of gram-negative bacte-
therapy and acute outcome of meningitis due to Streptococcuspneumoniae considered intermediately susceptible to broad-
13. Chiou CC, McEllistrem MC. Novel penicillin-, cephalosporin-,
spectrum cephalosporins. Antimicrob Agents Chemother
and macrolide-resistant clones of Streptococcus pneumoniae sero-
types 23F and 19F in Taiwan which differ from international
34. Rockowitz J, Tunkel AR. Bacterial meningitis: practical
epidemic clones. J Clin Microbiol 2001;39:1144–1147
guidelines for management. Drugs 1995;50:838–853
14. Rowe-Magnus DA, Mazel D. Resistance gene capture. Curr
35. Kollef MH, Sherman G, Ward S, Fraser VJ. Inadequate an-
timicrobial treatment of infections: a risk factor for hospital
15. Hall RM. Mobile gene cassettes and integrons: moving an-
mortality among critically ill patients. Chest 1999;115:462–474
tibiotic resistance genes in gram-negative bacteria. Ciba
36. Kollef MH. Inadequate antimicrobial treatment: an impor-
tant determinant of outcome for hospitalized patients. Clin
16. Arthur M, Reynolds P, Courvalin P. Glycopeptide resistance
in enterococci. Trends Microbiol 1996;4:401–407
37. Montravers P, Gauzit R, Muller C, Marmuse JP, Fichelle A,
17. Leclercq R, Courvalin P. Bacterial resistance to macrolide,
Desmonts JM. Emergence of antibiotic-resistant bacteria in
lincosamide and streptogramin antibiotics by target modifica-
cases of peritonitis after intraabdominal surgery affects the ef-
tion. Antimicrob Agents Chemother 1991;35:1267–1272
ficacy of empirical antimicrobial therapy. Clin Infect Dis
18. Hooper DC. Mechanisms of action of antimicrobials: focus on
fluoroquinolones. Clin Infect Dis 2001;32(suppl 1):S9–S15
38. Hanssen AD, Osmon DR. Assessment of patient selection
19. Gonzales RD, Schreckenberger PC, Graham MB, Kelkar S,
criteria for treatment of the infected hip arthroplasty. Clin
DenBesten K, Quinn JP. Infections due to vancomycin-resistant
Enterococcus faecium resistant to linezolid. Lancet 2001;357:1179
39. Mekontso-Dessap A, Kirsch M, Brun-Buisson C, Loisance D.
20. Tsiodras S, Gold HS, Sakoulas G, et al. Linezolid resistance
Poststernotomy mediastinitis due to Staphylococcus aureus: com-
in a clinical isolate of Staphylococcus aureus. Lancet 2001;358:
parison of methicillin-resistant and methicillin-susceptible
21. Oliver A, Canton R, Campo P, Baquero F, Blasquez J. High
40. Hyatt JM, Schentag JJ. Pharmacodynamic modeling of risk
frequency of hypermutable Pseudomonas aeruginosa in cystic
factors for ciprofloxacin resistance in Pseudomonas aeruginosa.
fibrosis lung infection. Science 2000;288:1251–1253
Infect Control Hosp Epidemiol 2000;21(suppl):S9–S11
SEMINARS IN RESPIRATORY AND CRITICAL CARE MEDICINE/VOLUME 23, NUMBER 5 2002
41. Sullivan A. Effect of antimicrobial agents on the ecological
60. Labarca J. Antibiotic cycling tested in nosocomial infections.
balance of human flora. Lancet Infect Dis 2001;1:101–114
42. Patterson JE. Antibiotic utilization: is there an effect on an-
61. Evans RS, Burke JP, Classen DC, et al. Computerized identi-
timicrobial resistance? Chest 2001;119(suppl):S426–S430
fication of patients at high risk for hospital-acquired infec-
43. Woodward RS, Medoff G, Smith MD, Gray JL III. Antibi-
otic cost savings from formulary restrictions and physician
62. Evans RS, Pestotnik SL, Classen DC, Burke JP. Development
monitoring in a medical-school-affiliated hospital. Am J Med
of an automated antibiotic consultant. MD Comput 1993;
44. Rahal JJ, Urban C, Horn D, et al. Class restriction of
63. Evans RS, Classen DC, Pestotnik SL, Lundsgaarde HP,
cephalosporin use to control total cephalosporin resistance in
Burke JP. Improving empiric antibiotic selection using com-
nosocomial Klebsiella. JAMA 1998;280:1233–1237
puter decision support. Arch Intern Med 1994;154:878–884
45. White AC Jr, Atmar RL, Wilson J, Cate TR, Stager CE,
64. Evans RS, Pestotnik SL. Applications of medical informatics
Greenberg SB. Effects of requiring prior authorization for se-
in antibiotic therapy. Adv Exp Med Biol 1994;349:87–96
lected antimicrobials: expenditures, susceptibilities, and clini-
65. Evans RS, Classen DC, Pestotnik SL, Clemmer TP, Weaver
cal outcomes. Clin Infect Dis 1997;25:230–239
LK, Burke JP. A decision support tool for antibiotic therapy.
46. Richardson LP, Wiseman SW, Malani PN, Lyons MJ, Kauff-
Proc Annu Symp Comput Appl Med Care 1995:651–655
man CA. Effectiveness of a vancomycin restriction policy in
66. Evans RS, Pestotnik SL, Classen DC, et al. A computer-
changing the prescribing patterns of house staff. Microb
assisted management program for antibiotics and other anti-
infective agents. N Engl J Med 1998;338:232–238
47. Leverstein-van Hall MA, Fluit AC, Blok HE, et al. Control
67. Hospital antibiotic control measures in the UK. Working
of nosocomial multiresistant Enterobacteriaceae using a tem-
Party of the British Society for Antimicrobial Chemotherapy.
porary restrictive antibiotic agent policy. Eur J Clin Microbiol
68. Shojania KG, Yokoe D, Platt R, Fiskio J, Ma’luf N, Bates
48. Yates RR. New intervention strategies for reducing antibiotic
DW. Reducing vancomycin use utilizing a computer guide-
resistance. Chest 1999;115(suppl):S24–S27
line: results of a randomized controlled trial. J Am Med In-
49. Patterson JE, Hardin TC, Kelly CA, Garcia RC, Jorgensen
JH. Association of antibiotic utilization measures and control
69. Wester C, Durairaj L, Schwartz D, Husain S, Martinez E,
of multiple-drug resistance in Klebsiella pneumoniae. Infect
Evans A. Antibiotic resistance who cares? Physician percep-
tions of antibiotic resistance among inpatients: its magnitude,
50. May AK, Melton SM, McGwin G, Cross JM, Moser SA,
causes, and potential solution [abstract 529]. In: Annual
Rue LW. Reduction of vancomycin-resistant enterococcal in-
Meeting of the Infectious Diseases Society of America. Phil-
fections by limitation of broad-spectrum cephalosporin use
adelphia: Infectious Diseases Society of America; 1999
in a trauma and burn intensive care unit. Shock 2000;14:259–
70. Murthy R. Implementation of strategies to control antimicro-
bial resistance. Chest 2001;119(suppl):S405–S411
51. Bassetti M, Di Biagio A, Rebesco B, Amalfitano ME, Topal
71. Thrasher CM, Stefl ME, Dorner FH. Antibiotic therapy in-
J, Bassetti D. The effect of formulary restriction in the use of
tervention at a community hospital: opportunities for cost
antibiotics in an Italian hospital. Eur J Clin Pharmacol 2001;
and quality improvements. Hosp Top 1995;73:12–15
72. Finkelstein JA, Metlay JP, Davis RL, Rifas-Shiman SL,
52. McGowan JE Jr. Do intensive hospital antibiotic control pro-
Dowell SF, Platt R. Antimicrobial use in defined populations
grams prevent the spread of antibiotic resistance? Infect Con-
of infants and young children. Arch Pediatr Adolesc Med
53. Durbin WA Jr, Lapidas B, Goldmann DA. Improved antibi-
73. Guillemot D, Maison P, Carbon C, et al. Trends in antimicro-
otic usage following introduction of a novel prescription sys-
bial drug use in the community—France, 1981–1992. J Infect
54. Kortas K, Segreti J, Donnelly A, Pierpaoli P, Trenholme G,
74. Nyquist AC, Gonzales R, Steiner JF, Sande MA. Antibiotic
Levin G. An anti-infective review and monitoring program.
prescribing for children with colds, upper respiratory tract in-
fections, and bronchitis. JAMA 1998;279:875–877
55. Thuong M, Shortgen F, Zazempa V, Girou E, Soussy CJ, Brun-
75. Zwar N, Wolk J, Gordon J, Sanson-Fisher R, Kehoe L. Influ-
Buisson C. Appropriate use of restricted antimicrobial agents in
encing antibiotic prescribing in general practice: a trial of pre-
hospitals: the importance of empirical therapy and assisted re-
scriber feedback and management guidelines. Fam Pract
evaluation. J Antimicrob Chemother 2000;46:501–508
56. Shlaes DM, Gerding DN, John JF Jr, et al. Society for
76. Finkelstein JA, Davis RL, Dowell SF, et al. Reducing antibi-
Healthcare Epidemiology of America and Infectious Dis-
otic use in children: a randomized trial in 12 practices. Pedi-
eases Society of America Joint Committee on the Prevention
of Antimicrobial Resistance: guidelines for the prevention of
77. Butler CC, Rollnick S, Kinnersley P, Jones A, Stott N. Re-
antimicrobial resistance in hospitals. Infect Control Hosp
ducing antibiotics for respiratory tract symptoms in primary
care: consolidating “why” and considering “how.” Br J Gen
57. Burke JP, Pestotnik SL. Antibiotic cycling: what goes around
comes around. Curr Opin Infect Dis 2000;13:367–369
78. Butler CC, Rollnick S, Pill R, Maggs-Rapport F, Stott N.
58. Kollef MH. Is there a role for antibiotic cycling in the inten-
Understanding the culture of prescribing: qualitative study of
sive care unit? Crit Care Med 2001;29:N135–142
general practitioners’ and patients’ perceptions of antibiotics
59. Evans RS, Pestotnik SL, Burke JP, Gardner RM, Larsen RA,
Classen DC. Reducing the duration of prophylactic antibiotic
79. Monnet DL, Sorensen TL. The patient, their doctor, the reg-
use through computer monitoring of surgical patients. DICP
ulator and the profit maker: conflicts and possible solutions.
Module Six is all about marketing. I’m going to share with you my experiences and what I’ve learned from running a thriving business. Nothing is a more powerful marketing tool than knowing who you are. That gives you a sense of confidence that is infectious. Your cake style is basically your business truth. It’s who you are. These days with so many gimmicks, being an open and honest business
Dres. María Inés Mota, Gustavo Varela, Br. María del Pilar Gadea y colaboradores ARTÍCULOS ORIGINALES Rev Med Uruguay 2005; 21: 30-36 Serotipos, perfil plasmídico y antibiotipos de cepas de Shigella flexneri aisladas de niños menores de 5 años con diarrea sanguinolenta usuarios de los servicios de Salud Pública Dres. María Inés Mota*, Gustavo Varela†, Br. María d
 EVOLUTION OF ANTIMICROBIAL RESISTANCE/GUILLEMOT ET AL
EVOLUTION OF ANTIMICROBIAL RESISTANCE/GUILLEMOT ET AL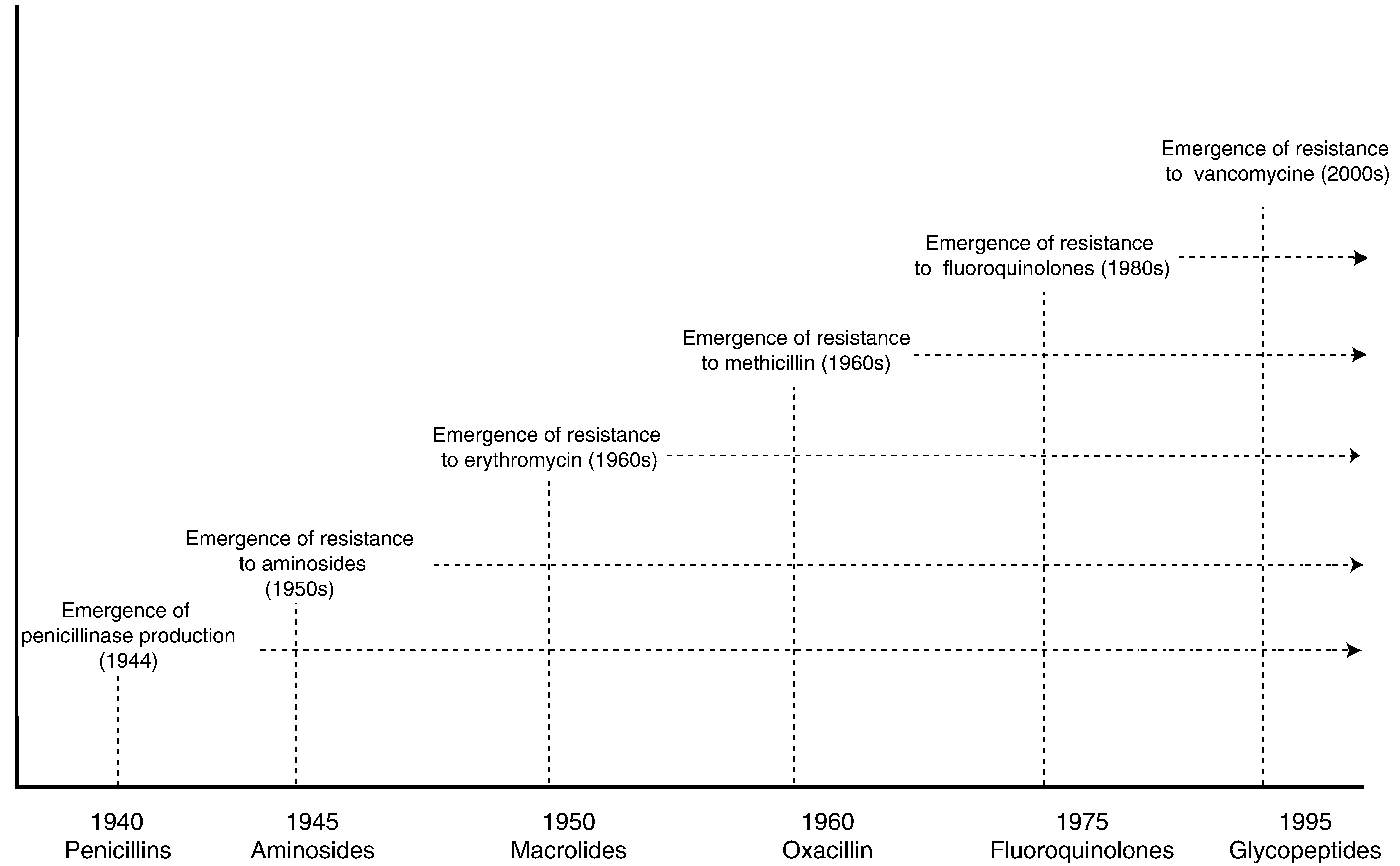 SEMINARS IN RESPIRATORY AND CRITICAL CARE MEDICINE/VOLUME 23, NUMBER 5 2002
SEMINARS IN RESPIRATORY AND CRITICAL CARE MEDICINE/VOLUME 23, NUMBER 5 2002