La spécificité du tadalafil est liée à sa longue demi-vie, permettant une action qui excède largement celle des autres inhibiteurs de PDE5. L’absorption digestive est complète, avec un pic plasmatique atteint en 2 heures environ. Le métabolisme est réalisé via CYP3A4, produisant des métabolites inactifs éliminés principalement dans les fèces. La sélectivité enzymatique est élevée, réduisant les effets indésirables extra-caverneux. Les réactions indésirables fréquentes incluent céphalées, bouffées vasomotrices et troubles digestifs légers. L’activité pharmacologique est stable, indépendamment de l’ingestion d’aliments. Dans les comparaisons de longue durée, acheter cialis pas cher est mentionné en relation avec les études portant sur la persistance d’efficacité et la constance de la cinétique plasmatique.
Impact of a new electronic handover system in surgery
Title: Impact of a new electronic handover system in surgery
Authors: S. Ryan, J.M. O'riordan, S. Tierney, K.C. Conlon, P.F. Ridgway
Received Date: 9 June 2010Revised Date: 29 October 2010Accepted Date: 23 November 2010
Please cite this article as: Ryan S, O'riordan JM, Tierney S, Conlon KC, Ridgway PF. Impact of a
new electronic handover system in surgery, International Journal of Surgery (2010), doi: 10.1016/
This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to
our customers we are providing this early version of the manuscript. The manuscript will undergo
copyediting, typesetting, and review of the resulting proof before it is published in its final form. Please
note that during the production process errors may be discovered which could affect the content, and all
legal disclaimers that apply to the journal pertain. IMPACT OF A NEW ELECTRONIC HANDOVER SYSTEM IN SURGERY
S RYAN, J M O’RIORDAN, S TIERNEY, KC CONLON & PF RIDGWAY
Department of Surgery, University of Dublin, Trinity College, Adelaide & Meath
Hospital Incorporating National Children’s Hospital, Tallaght, Dublin 24, Ireland
Running Title: Electronic Handover in Surgery
University of Dublin, Trinity College, Adelaide & Meath Hospital Incorporating National
Children’s Hospital, Tallaght, Dublin 24, Ireland
Changing patterns of workflow in the hospital setting have highlighted the
need for improvements in effective and safe handover of patient details. Financial
constraints mean that hospitals are under increasing pressure to maximise efficiency
and reduce length of stay of patients in hospitals and to reduce overtime bills for
junior doctors. The European Working Time Directive (EWTD) for junior doctors
also requires hospitals to comply with the 48 hour working week. This means the
introduction of a shift-based work practice for junior doctors and subsequently an
increased number of handovers between surgical on-call teams.
Continuity of information is imperative in order to reduce clinical risk and
maintain high standards of patient safety. Effectiv
and relevant information is transferred appropriately. In 2007, the Royal College of
Surgeons in England (RCSE) published gui Mregarding safe handover of patient
details1. Verbal and paper-based handovers are still common practice in many
institutions but the potential for clinical errors is significant. Electronic handover
systems, on the other hand, are suggested to provide better continuity of care than
To help improve clarity and efficiency of transfer of patient details between
surgical teams during handover post call, we recently introduced a bespoke, low-tech,
standardised template that could be used to record necessary patient information and
d through the hospital’s secure intranet to all relevant staff members. The
aim of this study was to prospectively audit the introduction of this new electronic
handover approach with particular emphasis regarding its efficacy and efficiency.
The primary surrogate chosen to assess efficacy and efficiency was length of stay for
those patients admitted through the emergency department. To do this we compared
two separate, two week periods before and after its introduction.
We analysed details of patient admissions through accident and emergency
during two separate time periods, each of two week duration, the first corresponding
to a period where written paper handover was used (n = 47) and the second following
the introduction of an electronic handover (n = 41). The particular time periods
coincided with the changeover of new interns to all surgical teams. The sample size
and study time periods were chosen for pilot validation. The Accident and
Emergency Department in our hospital is a tertiary referral centre seeing over 77,000
patients per year. The department of Surgery comprises six surgical specialties
including paediatrics. The total number of surgical emergency admissions per year is
A standardised template for the electronic h
with recent guidelines regarding safe hand M mind1. A mock example is given
below (Figure 1). Specifically, patient name, hospital number, location, age,
consultant in charge, time of referral, brief past medical history, presenting complaint,
investigation results available, examination findings, differential diagnosis and
management plan were detailed. Transfer of information to other surgical staff was
achieved using a secure email on the hospitals intranet service. Each participating
doctor had their own hospital email account (based only on the hospitals intranet)
which was easily accessible. This helped ensure patient confidentiality was upheld.
individual within the department was appointed as account administrator
and was able to add or remove group members accounting for the periodic staff
changes. The on-call team during each 24 hour period (8am to 8am) includes a
consultant, registrar and SHO. The SHO remains in house throughout the night
admitting patients from the emergency department. The registrar is available on call
on-site during normal daily working hours and from home after hours. The Senior
House Officer (SHO) on-call compiled the details of all patients admitted during a
full 24 hour period on call into the standardised template as detailed above. This was
then emailed to all surgical staff before commencement of the next days shift so that
all members of staff were informed prior to start of the next working day. In addition
a verbal handover also took place at the start of the next working day to discuss all
handover details. The SHO on call was not required to attend the post take ward
round. No other formal handover was performed.
The length of stay for all patients admitted during each two week period was
calculated. In addition we compared differences in ASA grades and admission
diagnosis to ensure that there were no significant di
of admissions during the two time periods studied. Finally, we also analysed time to
first intervention post admission. We chose Manning as the intervention as it was
possible to calculate in hours from time of admission to time of scan with accuracy.
This radiological investigation is generally available throughout the week as
compared to ultrasound for example which is not routinely available during weekends
in our hospital. To limit the possibility of Hawthorne effect4 influencing our findings
on length of stay, such that participants in the study might have improved an aspect of
their behaviour being experimentally measured in response to the fact that they were
being studied and not in response to any particular experimental manipulation,
doctors were unaware of the proposed audit intention following the
introduction of this electronic handover format in our department.
The particular time periods studied coincided with the changeover of new
interns to all surgical teams. Data collated from patients admitted while written
paper handover was still used was obtained during the first two weeks of April three
months prior to the introduction of electronic handover. We are mindful that a
potential bias against the introduction of the electronic handover may have occurred
as a result of the timing of its introduction however. Specifically, this took place
during the first week of July, a time period which coincides with introduction of new
junior doctors unfamiliar with the hospital so that we may have expected longer
patient hospital stay. Nevertheless, the two week control period where verbal/written
handover was investigated also coincided with a change of staff. In particular, this
involved changeover of intern doctors in the team.
Non-parametric data were analysed using Fisher’s exact test for 2 by 2
contingency tables and the Mann-Whitney U-test. For parametric data, an unpaired t
test was used for comparison of differences betwee
significance was ascribed to a p-value of less than 0.05. All data are reported as
medians and interquartile ranges unless othe Mtated.
We found that following the introduction of the electronic handover there was
a significant reduction in median length of stay (Fig 2, P = 0.047)compared with
patients admitted during a separate time period where paper handover was used. The
median length of stay was reduced from five to four days.
There was no significant confounding difference in patient ASA grade (P >
0.05). The admission case mix was also analysed for confounders. We separated
admissions into 6 categories. These included gastrointestinal (GI) neoplasms,
appendicitis, Upper/Lower GI conditions (pancreatitis, acute cholecystitis, bilary
colic, diverticulitis, bowel obstruction/perforation), vascular, trauma, and others
(gynaecology, non-specific abdominal pain (NS
significant difference between admission diagnosis was that for gastrointestinal (GI)
cancers where there was a significantly gr Mumber admitted during the period
where paper handover was still being utilised compared to that following the
introduction of electronic handover (Fig. 3, P < 0.05). However when these patients
were removed from the data interpretation, median length of stay remained
significantly shorter following introduction of electronic handover.
Finally, there was no significant difference in the time taken to obtain the first
intervention (Fig. 4) when both time periods were analysed before and after the
introduction of the electronic handover (P = 0.059, 21.2 ± 10.3 versus 28.2 ± 7.8
± SEM)). Of the 47 admissions pre-introduction of the electronic
handover, eight patients required CT scans (17%) whereas 24% obtained a CT scan
following its introduction (10 of 41 patients).
The results from this study support the use of electronic handover to improve
efficiency of patient information transferred between doctors. Furthermore, it
supports the continued use and development of this electronic format for handover
particularly as it serves as a user-friendly, low-cost, efficient means of transfer of
patient details among staff post-call leading to better continuity of care for patients.
Importantly, this is the first study to show that use of electronic handover is associated
with a significant reduction in patient length of stay. This is despite the pilot nature of
Traditionally, verbal communication of handover details has been common
practice often supported with the use of hand-writt
that this mechanism is far from ideal as important information may not be transmitted
consistently or legibly and represents a rea Mo our patients’ quality of care. An
electronic handover system represents a potential solution. The Royal College of
Surgeons of England recently published guidelines1 with regards minimum handover
requirements in order to convey high quality clinical information and allow for the
safe transfer of responsibility for patients. Following the 2004 Hospital at Night pilot
studies covering four NHS trusts6 it was recommended that handover could be
enhanced if it was more IT driven. In support of this, Raptis et al1 demonstrated that
electronic handover provides better continuity of care than paper based handover.
al3 showed that the introduction of electronic handover using secure
email resulted in improved handover consistency and helped to prevent
miscommunication. Others have shown, however, that electronic handover using a
system requiring input of free text entry was associated with occasional deficiencies
in important handover information and recommended that the use of prompts or
predefined fields for information provision may further minimise inadequate
information transfer5. We feel our templated format is a good medium between the
rigid nature of prompted entries and the loose nature of free text. The delivery to the
care practitioner is an essential point. We feel that without this the system would not
be used. Therefore, login sites where the practitioner has to go to search for the
information would negatively bias this form of information transfer.
To date it has not been shown whether improvements in quality of information
transfer at handover translates into more effective and efficient management of patient
care. The present study is the first to demonstrate a significant reduction in patient
length of stay following the introduction of electronic handover. These results could
not be explained by differences in ASA grades or a
significant difference between groups for either of these potential confounders. It is
noted that our patient groups consisted of s Mutliers, particularly those in the GI
cancer groups with associated individual longer lengths of stays. Although the
reduction in length of stay remained significantly different when these patient groups
were removed from the analysis, it may be warranted in future studies of this new
handover system to include larger sample sizes to elucidate this point. We also
examined whether improved patient handover may have resulted in quicker and more
efficient planning of in-patient care. Specifically, we assessed the time taken to obtain
first radiological investigation and hypothesised that a reduction in time to first
may contribute to a reduction in length of stay. We found, however, no
significant difference in time to first intervention between the two groups studied. It is
noted that the low number of CT scans obtained in both groups may have accounted
for failure to detect any significant difference and it is a limitation of the current work
that results are based on a pilot study looking at a limited time period following the
introduction of the electronic handover. Nevertheless, given the timing of introduction
of the electronic handover during the first two weeks in July, a time period which
coincides with introduction of junior doctors unfamiliar with the hospital, we may
have expected longer patient hospital stay. We are also mindful that length of stay in
hospital for surgical patients is impacted by many different factors such as
complications, social circumstances and disease severity. With regards the latter, we
have shown no significant difference in overall admission diagnosis between groups.
Nevertheless, the increased clarity and consistency of handover information post call
resulted in each team member having ready access to review reliable, accurate and
pertinent details regarding new patient admissions including diagnosis and
management plan together with results of prel
already during the period of on-call and detailed on every handout post-call. This led
to a clearer and early understanding of the Mment plan required for each patient
by each member of the team. Our data thus far, however, does not allow us draw
robust conclusions with regards this and further study is required to examine
specifically which factors may have contributed to our findings.
The need to maintain continuity of patient care and reduce risk for potential
clinical errors is particularly relevant given the recent introduction of the EWTD with
the move towards shift patterns, thereby increasing the number of different
individuals caring for patients and subsequently an increased potential for error. As a
h measures, the provision of comprehensive and efficient communication
of patient details at handover is increasingly important. The handover format used in
the present study required SHO doctors on call to list their differential diagnosis for
each patient admitted. Although, not specifically addressed in our analysis, this
requirement has the potential to be utilised as an important teaching tool whereby
feedback from seniors including admitting consultant and affiliated registrars could be
made to SHOs regarding their admitting diagnosis on-call, how that conclusion was
made, and comparing this to the actual diagnosis for each patient.
In conclusion, accurate post-call doctor-to-doctor handover is vital to protect
patient safety. Our findings support the used of templated electronic handover as an
enhancement of efficient transfer of patient details. To our knowledge, this is the first
study to show that the introduction of electronic signout post call was associated with
a significant reduction in patient length of stay.
1. The Royal College of Surgeons of England (2007). Safe Handover: guidance
from the Working Time Directive Working Party, RCSE, London.
(http://www.rcseng.ac.uk/publications/docs).
2. Raptis DA, Fernandes C, Chua W & Boulos PB (2009). Electronic software
significantly improves quality of handover in a London teaching hospital. Health
3. Stimpson P, Joshi A, Oakley R & Simo R (2009). Surgical Handover: aspiring to
easy access without breach of patient confidentiality. Clin Otolaryngol 34, 83-84.
4. Adair, G (1984) The Hawthorne effect: A reconsideration of the methodological
artifact. Journal of Appl. Psychology 69 (2), 33
5. Cheah LP, Amott DH, Pollard J & Watters DAK (2005). Electronic medical
handover: towards safer medical care. Ml J Australia 183(7); 369-372.
6. MacDonald R & Eccles S (2004). The hospital at night. BMJ Career Focus 328;
Figure 1. Mock example of templated email handover details Figure 2. Box-plot graph and quartile ranges for median length of stay.
Graph shows the median length of stay (horizontal shaded bar) and quartile range
together with outliers in each group for the two week period paper-handover was used
(pre-signout) and that during a second two week period in July following the
introduction of electronic handover (post-signout). († indicates a statistically
Figure 3. Case mix of admissions pre- and post-si
Graph showing case mix of admissions fro Memergency department. The open
columns represent admissions during a two week period in April during which paper
handover was used. The filled columns represent admissions during the first two
weeks following introduction of the electronic handover. * indictates statistically
Figure 4. Time to first intervention pre- and post-signout.
Graph illustrating the time in hours (mean ± SEM) to CT scan post admission. The
s represent admissions during a two week period in April during which
paper handover was used. The filled columns represent admissions during the first
two weeks following introduction of the electronic handover.
DATE: 21/12/12 TEAMS On Call: General Consultant Surgeon: Mr PFR Vascular Consultant Surgeon: Prof ST Senior Registrar:Mr M S SHO: Dr S R STATS:
Patients brought to Theatre:
A&E ADMISSIONS: 1. J Smith, 82yr old, MRN: 666110, Ward: Gogarty Bed: 4-4, Consultant: Mr PFR Paged 17:45, Seen 18:15, Plan 19:20 Background: dementia, Hx of diverticulosis. Presenting Complaint: Transferred from nursing home for kneeA and NabdoUSCRIPT Investigations: CXR read by staff radiologist as ?free air. WCC 43, CRP 230. On Examination: hypotensive, Abdomen rigid. Impression: Bowel Perforation PLAN: Resuss, Theatre, cipro/flagyl iv antibiotics. Frequency Diagnosis imeto1stIntervention T Admission Period
DIABETES CONTROL MATTERS A CLOSER LOOK AT ORAL AGENTS FOR THE PATIENT Today, there are several kinds of oral agents, ordiabetes pills, available for the treatment of type 2diabetes. If you have type 2 diabetes, your doctorand health care team can help you decide which oralagent or combination of oral agents are the best foryou. Here are some general tips about oral agents:• Many doctor
QIAGEN Plasmid Maxi Prep Things to do before starting • Make sure RNase A solution has been added to Buffer P1. • Check Buffer P2 for SDS precipitation • Optional: Add LyseBlue reagent to Buffer P1; 1:1000 dilution; see notes below Grow Bacterial culture Inoculate 100mls (high copy number plasmids) to 500mls (low copy number plasmids- see note for chloramphenicol) from glyc
 Title: Impact of a new electronic handover system in surgery
Authors: S. Ryan, J.M. O'riordan, S. Tierney, K.C. Conlon, P.F. Ridgway
Received Date: 9 June 2010Revised Date: 29 October 2010Accepted Date: 23 November 2010
Please cite this article as: Ryan S, O'riordan JM, Tierney S, Conlon KC, Ridgway PF. Impact of a
new electronic handover system in surgery, International Journal of Surgery (2010), doi: 10.1016/
This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to
our customers we are providing this early version of the manuscript. The manuscript will undergo
copyediting, typesetting, and review of the resulting proof before it is published in its final form. Please
note that during the production process errors may be discovered which could affect the content, and all
legal disclaimers that apply to the journal pertain.
Title: Impact of a new electronic handover system in surgery
Authors: S. Ryan, J.M. O'riordan, S. Tierney, K.C. Conlon, P.F. Ridgway
Received Date: 9 June 2010Revised Date: 29 October 2010Accepted Date: 23 November 2010
Please cite this article as: Ryan S, O'riordan JM, Tierney S, Conlon KC, Ridgway PF. Impact of a
new electronic handover system in surgery, International Journal of Surgery (2010), doi: 10.1016/
This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to
our customers we are providing this early version of the manuscript. The manuscript will undergo
copyediting, typesetting, and review of the resulting proof before it is published in its final form. Please
note that during the production process errors may be discovered which could affect the content, and all
legal disclaimers that apply to the journal pertain.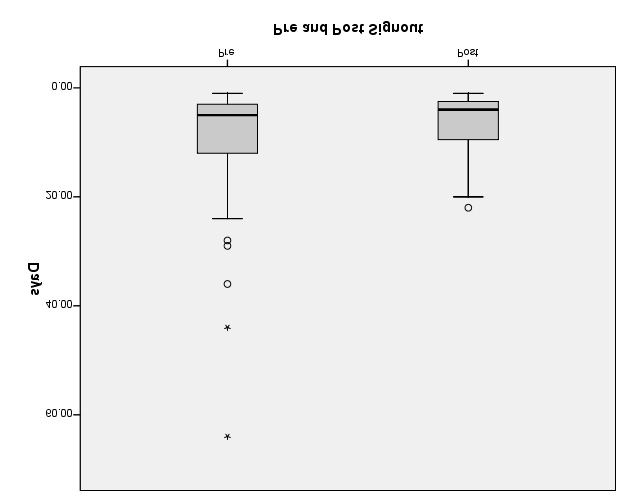 Frequency
Frequency