La spécificité du tadalafil est liée à sa longue demi-vie, permettant une action qui excède largement celle des autres inhibiteurs de PDE5. L’absorption digestive est complète, avec un pic plasmatique atteint en 2 heures environ. Le métabolisme est réalisé via CYP3A4, produisant des métabolites inactifs éliminés principalement dans les fèces. La sélectivité enzymatique est élevée, réduisant les effets indésirables extra-caverneux. Les réactions indésirables fréquentes incluent céphalées, bouffées vasomotrices et troubles digestifs légers. L’activité pharmacologique est stable, indépendamment de l’ingestion d’aliments. Dans les comparaisons de longue durée, acheter cialis pas cher est mentionné en relation avec les études portant sur la persistance d’efficacité et la constance de la cinétique plasmatique.
Microsoft word - new patient packet without opiate agreement.doc
Alpine Medical Group LLC, Pain Management Division
Steven Pulley, MD ■ Nathan Dahle, MD ■ Thomas Trauba, MD ■ N. Lee Smith, MD
■ Whitney Bancroft, APRN ■ Katie Toledo, APRN, FNP ■ Laura Chamberlain, MSN, NPC
Welcome Valued Patients to Omega Interventional Pain Clinic! As of January 1, 2011 the following are Patient Guidelines for All existing as well as New Patients effective immediately:
• For your continued safety and comfort we advise using interventions to reduce medication use. • Patients requiring muscle relaxants will be given Flexeril, Zanaflex, Robaxine, etc…NOT Soma. • You must have a Primary Care Physician, internist, Family Practice Physician or specialist for all prescriptions not pain related – i.e. blood pressure, diabetes, insomnia, depression etc…
• Any patient failing his or her urine drug screen will required 1 week Follow Up visit. At that time your provider will determine if you are to receive any prescriptions that week.
• Benzodiazepine prescriptions must be approved by Dr. Trauba or other Psychiatrist and will continue to be prescribed only by that physician. They will not be prescribed for sleep.
• No initiation or prescription assumption for respiratory depressing sleep aids. • You will receive only 1 short acting Opioid and only1 long acting Opioid, not to exceed 150mg Morphine equivalent per day. EVERYONE with doses above 100mg Morphine equivalent must have a documented sleep study for your safety.
• Anyone having an Upper Respiratory Infection or pneumonia must reduce their Opioids by 1/3 and stop use at
• Anyone that is not compliant with their treatment for sleep apnea will require stopping their Opioids. • Patients on long term Opioid therapy should be evaluated by a Psychiatrist for the psychiatric effects of chronic
• Any patient who overuses or loses an Rx or medication will not be given early refills. • Patients who need higher doses of medications need to be considered for possible alternatives ie: Intrathecal
• Exercise can and should be used as an additional form of conditioning. Date: __________________ Patient Signature indicating I have read and will comply by these guidelines _____________________________________________
Alpine Medical Group LLC, Pain Management Division
PATIENT ACCOUNT TERMS Regarding payment of your bill Billing: Upon admission to Omega Interventional Pain Clinic, you have contractually agreed to pay for services rendered to you. If you have Health Insurance coverage, Omega will agree to file your initial claim(s), provided we have complete insurance information and your Insurance forms at the time of admission (if forms are required). However, your health insurance contract(s) are between you and the insurance carrier. Because of this relationship, you have primary responsibility to pay for services and provide follow-up communication with your health insurance carrier (s), if necessary. Should your health insurance reject our claim for any reason, you are financially responsible. If your health insurance coverage requires the insured to pay a deductible and percentage or a copay, these amounts will be due the day of service. We will try to give you an estimate of the amount you may owe before your visit. Payment can be made by cash, check, Visa, Mastercard, Discover Card, or American Express. If you do not have health insurance you will be required to pay for all services at the time they are received. Liens will Not be Accepted under any circumstances. Missed Appointments: Any appointments not cancelled with a 24-hour notice will be assessed a fee, $50.00 for a follow-up evaluation and $100.00 for any scheduled procedure. Medicare: Omega participates with Medicare and will accept what Medicare allows. Omega will bill Medicare for you. However, Medicare is a co-pay carrier, which means they will pay 80% of the allowed charges. You will be responsible for 20% of the allowed charges plus any deductible. These amounts will be due the day of service unless you have a supplementary insurance. Agreement: I have acknowledged that I understand and have received a copy of this notice. I agree to make payment for services rendered by Omega Interventional Pain according to the above terms. I authorize my Insurance to send payment directly to Omega Interventional Pain. I agree to pay and finance charge of one and half percent (1 ½ %) per month on all amounts due to and owing to Omega Interventional Pain. Attorney’s Fees & Costs: If any legal action is necessary to enforce the terms of this Agreement, or if it is necessary to employ the services of an attorney to enforce the terms of this agreement, the party in default or in breach hereof agrees to pay the other party’s reasonable attorney’s fees and court costs n addition to any other relief to which it may be entitled if I fail to pay any amounts owing hereunder when due, or otherwise breach any terms of this agreement. I agree to pay up to 50% collection expense incurred by Omega Interventional Pain in attempting to collect such amounts from me, in addition to the aforementioned attorney’s fees and costs. Responsible Party:____________________________
Patient Signature:____________________________
Alpine Medical Group LLC, Pain Management Division
Steven Pulley, MD ■ Nathan Dahle, MD ■ Thomas Trauba, MD ■ N. Lee Smith, MD
■ Whitney Bancroft, APRN ■ Katie Toledo, APRN, FNP ■ Laura Chamberlain, MSN, NPC
Patient______________________________ Account #_______________ Date_______________ Physician/Supplier Notice: Your insurance will only pay for services that it determines to be “reasonable and necessary.” If your insurance
determines that a particular service, although it would otherwise be covered, is not “reasonable and necessary” under your
insurance program standards, they could deny payment for that service. With regard to your insurance they could deny
payments for Office Visits & Clinical Procedures for one of the following reasons: 1. Not a covered benefit 2. Not medically necessary
Even though prior authorization has been obtained and verification of benefits and coverage has been verified, the above
Beneficiary Agreement:
“I have been notified by my physician/supplier that he or she believes that, in my case, my insurance could deny payment
for the services identified above, for the reasons stated. If my insurance denies payment, I agree to be personally and fully
Patient Signature:___________________________________ Date:____________________
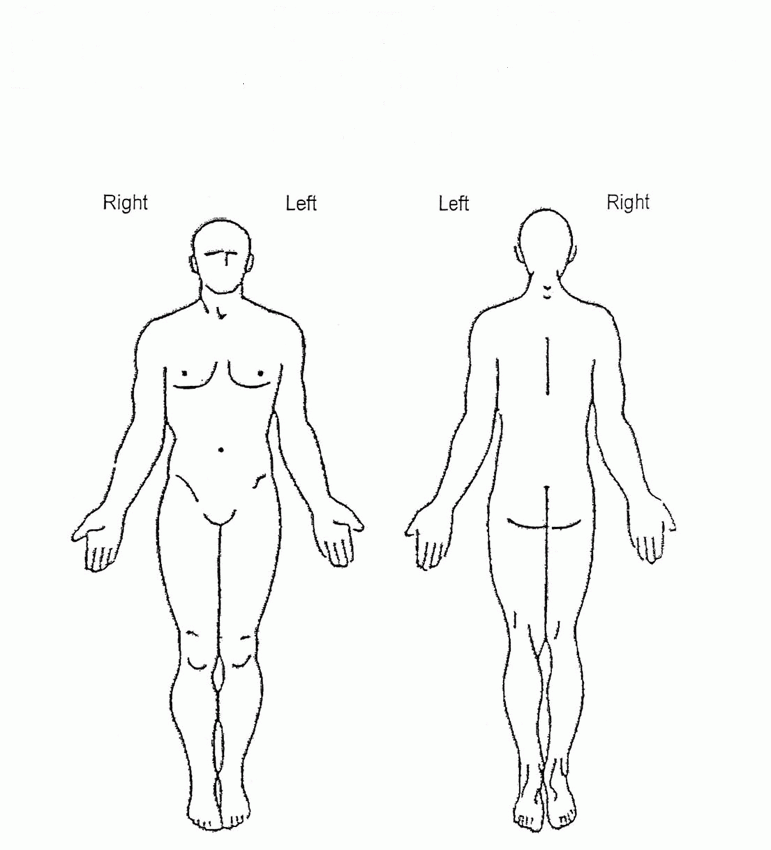
Please indicate the areas you are having pain
How long have you had this pain?_____________________________________________________________
Was there an initiating event?___________________________________________________________
What makes your pain worse?__________________________________________________________________ What makes your pain better?__________________________________________________________________
How would you describe your pain (circle all that apply)? Aching Throbbing Shooting Burning Pins and Needles Stabbing Sharp Cutting Gnawing Cramping Tugging Pulling Hot Searing Tingling Itching Stinging Tender Taut Tiring Exhausting Annoying Troublesome Miserable Intense Unbearable Radiating Tight Numb Squeezing Tearing Cold Nagging Nauseating Agonizing Dreadful Circle the number that best describes your baseline or constant level of pain
Circle the number that best describes your lowest level of pain
Circle the number that best describes your worst level of pain
Pain Medication Have you been given opioid (narcotic) medication for your pain? Yes No If yes, have they improved your activity or general level of function?
Do you feel your doctor is reluctant to prescribe opioids?
Are you concerned about addiction if you are prescribed opioids?
Are any members of your family concerned about addiction if your are prescribed opioids?
What pain medications have you taken in the past? Vicodin
Have you ever had the following types of treatment for your PRESENT pain problem(s) and what was the result?
Other local anesthetic or Steroid Injections
Have you had any of the following tests for your pain? Blood Tests
Medications previously tried: Medication
Function:
What areas of your life have been affected by your pain? (Circle all that apply)
Mood: Do you feel: blue, depressed, down, or hopelessness due to pain?
Do you feel anxious or nervous due to your pain?
Do you have thought of harming yourself?
Are you currently or have you ever been under the care of a mental heath specialist (Psychiatrist or
Psychologist)? Sleep:
How many hours doe you sleep at night?
How many times do you awaken at night due to pain?
What Surgeries have you had in the past? Name of Surgery What Other Medical Conditions do you have? 1 Please list all prescription medications your are taking: Name
Do you take any blood thinners like Coumadin, Plavix, or Lovenox? Please list all other nonprescription medication you are taking (e.g., Tylenol, Advil, Aleve, Vitamins, herbal supplements, homeopathic remedies, etc.)____________________________________________________________ ______________________________________________________________________________________________________ Allergies: (an allergy means a rash, swelling, difficulty in breathing. It does NOT mean causing stomach upset or dizziness) Are you allergic to any medication?
If yes, Please list the medication and your reaction to the medication: Medication:
Social History: Do you Smoke?
What type of alcohol?___________________
Do you/have you ever used drugs or prescriptions
that were not yours? Have you ever received Alcohol or Drug Addiction
Family History: Is there a history of chronic
pain syndromes? Please List any other medical
conditions that run in your family: Review of Systems: (Circle all that apply): Review of Systems (cont’d) Musculoskeletal Neurologic Psychiatric
For Office Use Only: Assessment:_________________________________________________________________________ ___________________________________________________________________________________ ___________________________________________________________________________________ ___________________________________________________________________________________ ___________________________________________________________________________________ ___________________________________ Plan:_______________________________________________________________________________ ___________________________________________________________________________________ ___________________________________________________________________________________ ___________________________________________________________________________________ ___________________________________________________________________________________ ___________________________________
Scientific and Referred Dental Journal Vol.11No.1,2011 Al–Rafidain Dental Journal E ffect of Thickness and Recycling on Transverse Strength of Relined Acrylic Resin Denture Base. Hatim NA, AL-Omari AW ------------------------------------------------------------------------------------1-5. E lasticity and Plasticity Behaviors of the Orthodontic Arch Wires Obaidi HA, Al-Qassar SS
Corona® CAD® - Charged Aerosol Detector Comparable Response Between AnalytesDuring Gradient Elution HPLC Using A Make-upInverse Gradient The response of nebulization-based detectors A ilent 12 typically varies as a function of mobile phasevolatility. An increase in the organic content ofthe eluent leads to more efficient nebulization,an increase in the percentage of analyte reac
 Please indicate the areas you are having pain
How long have you had this pain?_____________________________________________________________
Was there an initiating event?___________________________________________________________
What makes your pain worse?__________________________________________________________________ What makes your pain better?__________________________________________________________________
How would you describe your pain (circle all that apply)?
Please indicate the areas you are having pain
How long have you had this pain?_____________________________________________________________
Was there an initiating event?___________________________________________________________
What makes your pain worse?__________________________________________________________________ What makes your pain better?__________________________________________________________________
How would you describe your pain (circle all that apply)?