La spécificité du tadalafil est liée à sa longue demi-vie, permettant une action qui excède largement celle des autres inhibiteurs de PDE5. L’absorption digestive est complète, avec un pic plasmatique atteint en 2 heures environ. Le métabolisme est réalisé via CYP3A4, produisant des métabolites inactifs éliminés principalement dans les fèces. La sélectivité enzymatique est élevée, réduisant les effets indésirables extra-caverneux. Les réactions indésirables fréquentes incluent céphalées, bouffées vasomotrices et troubles digestifs légers. L’activité pharmacologique est stable, indépendamment de l’ingestion d’aliments. Dans les comparaisons de longue durée, acheter cialis pas cher est mentionné en relation avec les études portant sur la persistance d’efficacité et la constance de la cinétique plasmatique.
Electroretinography in the western gray kangaroo (macropus fuliginosus)
Veterinary Ophthalmology (2010) 13, Supplement 1, 41–46
Electroretinography in the western gray kangaroo(Macropus fuliginosus)
Amber L. Labelle,* Ralph E. Hamor,* Kristina Narfstro¨m† and Carrie B. Breaux*,1*Department of Veterinary Clinical Medicine, Veterinary Teaching Hospital, Urbana, Illinois; †Ruth M Kraeuchi Endowed Professor Emeritus of VeterinaryOphthalmology, Columbia, Missouri
Objective To perform electroretinography on normal anesthetized western graykangaroos (Macropus fuliginosus).
Animals studied Six captive western gray kangaroos.
Procedures The kangaroos were anesthetized using a combination of ketamine andmedetomidine via a remote drug delivery system, then were maintained on isoflurane
after endotracheal intubation and reversal of the medetomidine with atipamazole.
Animal Emergency andSpecialty Center, 5019 N.
After a minimum of 20 min of dark adaptation, electroretinograms were obtained
using a handheld electroretinography (ERG) machine using a single flash protocol at
three light intensities: 10 mcd.s/m2, 3000 mcd.s/m2, 10 000 mcd.s/m2. Results At 10 mcd.s/m2 the mean b-wave amplitude and implicit time was 102.0 lV(SD ± 41.3 and 95% CI 68.9–135.1) and 78.4 ms (SD ± 8.3 and 95% CI 71.8–85.0). At 3000 mcd.s/m2 the mean a-wave amplitude and implicit time was 69.9 lV(SD ± 20.5 and 95% CI 53.5–86.3) and 17.6 ms (SD ± 1.5 and 95% CI 16.4–18.8)and the mean b-wave amplitude and implicit time was 175.4 lV (SD ± 35.9 and 95%CI 146.7–204.1) and 74.1 ms (SD ± 3.5 and 95% CI 71.2–76.9). At 10 000 mcd.s/m2the mean a-wave amplitude and implicit time was 89.1 lV (SD ± 27.1 and 95% CI67.5–110.8) and 16.8 ms (SD ± 1.0 and 95% CI 16.0–17.0) and the mean b-waveamplitude and implicit time was 203.7 lV (SD ± 41.4 and 95% CI 170.6–236.8) and75.4 ms (SD ± 3.3 and 95% CI 72.8–78.1). Conclusion Electroretinography outside of the typical clinical setting is feasible using aportable ERG system and allows for quick analysis of retinal function in exoticspecies.
Key Words: electroretinogram, eye, macropod, Macropus fuliginosus, retina, westerngray kangaroo
a-wave is produced by the hyperpolarization of photorecep-
tors as they undergo phototransduction, whereas the b-wave
Electroretinography (ERG) is commonly utilized in veteri-
is produced primarily by bipolar cells.6–8 Traditional ERG
nary ophthalmology to assess and document retinal electri-
units are bulky and nonportable, however within the last
cal function. The first reports of canine and feline ERGs
10 years several portable ERG systems have become com-
occurred in the early and mid 20th century.1–3 ERG is used
mercially available, making electrodiagnostic assessment of
in research settings for the study of inherited and acquired
nontraditional patients possible outside of the traditional
retinopathies, in clinical settings for differentiating retinal
research laboratory or clinical setting.
vs. central nervous system disease in cases of acute vision loss
Western gray kangaroos (Macropus fuliginosus) are macro-
and for evaluating retinal electrical function in patients with
pods native to Southwestern Australia. With weights from
opaque ocular media that precludes direct examination of
28 to 54 kg, heights up to 1.1 m, and tail lengths from 80 to
the posterior segment.4,5 The ERG represents a complex
100 cm, they are one of the largest species of kangaroo.
summation of electrical potentials and currents generated
Males are generally twice as large as females, however they
within the cells of the retina. The negative deflection of the
are all herbivorous. Although western gray kangaroos are
Ó 2010 American College of Veterinary Ophthalmologists
commonly housed in zoological collections, there is a
then blindly intubated using a 6.0 or 7.0 mm internal diame-
paucity of information about the normal ophthalmic
ter endotracheal tube, and isoflurane was continuously
examination findings and common ocular diseases of this
administered at concentration of 1–3% with 2–3 L/min of
species. Published reports include a review of common mar-
oxygen. Atipamazole (Antisedan; Pfizer Animal Health) was
supial ocular diseases, a single report of retinal degeneration
then administered intramuscularly at a dose of five times that
in a Goodfellow’s tree kangaroo (Dendrolagus goodfellowii)
of the previously administered medetomidine, and the kan-
and several detailed descriptions of a viral outbreak of ante-
garoo was maintained on isoflurane during the ERG. The
rior uveitis, chorioretinitis, optic neuritis and encephalitis
amount of time between administration of the atipamazole
causing vision loss in Australian kangaroos.9–13 A review of
and the start of the ERG varied from 10 to 16 min.
normal ocular examination findings in a captive mob of wes-
Atipamazole is reported to reverse sedation and analgesia in
dogs within 5–10 min, and these effects are extrapolated in
A retrospective evaluation of necropsy data on kangaroos
western gray kangaroos as no pharmacologic studies are
housed in a single zoological collection revealed a high prev-
available in this species.18 After conclusion of the ERG
alence of histologic lesions compatible with hypertension,
and all additional anesthetic monitoring, administration of
including renal arteriolar smooth muscle hypertrophy,
isoflurane and oxygen was discontinued and the kangaroos
extracellular matrix accumulation within renal arterioles,
were moved to a dark and quiet recovery area where
renal vascular tortuosity, juxtaglomerular hyperplasia and
extubation was performed at the first sign of swallowing or
hypertrophy of arterioles and arteries in both the retina and
purposeful movement. No regurgitation or vomiting was
central nervous system.15 Hypertension is frequently associ-
ated with retinopathy, particularly in the cat.16 A recent
Each kangaroo in this study had received a complete oph-
report identified decreased b-wave amplitudes in spontane-
thalmic examination under general anesthesia 3 months
ously hypertensive rats.17 Establishing a protocol for ERGs
prior to this study. Complete ophthalmic examination
in western gray kangaroos may be a useful part of evaluating
included diffuse illumination, slit lamp biomicroscopy
a mob for hypertension and its associated ocular lesions.
(Kowa-SL2; Kowa, Tokyo, Japan), and indirect funduscopy
The goal of this study was to demonstrate a method for per-
(Keeler Instruments Inc., Broomall, PA, USA) with a 2.2D
forming ERGs in an exotic species in a nonclinical setting.
handheld condensing lens (PanRetinal 2.2; Volk Optical,Inc., Mentor, OH, USA). Intraocular pressure (IOP) wasestimated using rebound (Tonovet; Icare Finland Oy,
Espoo, Finland) and applanation tonometry (Tonopen-XL;
The study protocol was approved by the Brookfield Zoo
Research and Scientific Committee and Institutional Animal
No ophthalmic abnormalities were observed in any kan-
Care and Use Committee. A mob of six captive adult wes-
garoo included in the ERG study group that could poten-
tern gray kangaroos (three males and three females) were
tially impact the ERG. Observed abnormalities did include a
included in the study, ranging in age from 3 to 7 years and in
subepithelial scar, incipient anterior cortical cataract, eyelid
weight from 22.4 to 67.5 kg. All kangaroos were considered
notch defect, nuclear sclerosis and vitreal degeneration. One
to be in good health at the time of the study with no evidence
kangaroo in the mob was observed to have a regional focal
of visual deficits. Each kangaroo was anesthetized using a
choroidal hypoplasia and an optic nerve coloboma, however
remote drug delivery system (Telinject; Telinject USA, Inc.,
that kangaroo was not included in this study.14
Agua Dulce, CA, USA) with 2 mg/kg ketamine hydrochlo-
Since all kangaroos had been examined 3 months prior to
ride (Ketaset; Fort Dodge Animal Health, Fort Dodge, IA,
this study, complete ophthalmic examination was not per-
USA) and 50 lg/kg medetomidine hydrochloride (Domitor;
formed prior to the harvesting of ERGs in this study to avoid
Pfizer Animal Health, Exton, PA, USA) administered intra-
the deleterious effects of excessive light exposure on the
muscularly with doses based on the most recently available
ERG.19 Tonometry with applanation and rebound tonome-
body weight of the animal (information no older than
try was performed prior to the instillation of tropicamide
3 months for any kangaroo). The anesthetic drugs were
1% solution (Tropicamide 1% USP; Alcon Laboratories,
administered within the kangaroo enclosure while the ani-
Inc., Fort Worth, TX, USA) for mydriasis. Dark adaptation
mals were free-ranging, and when the kangaroo became
times varied from 20 to 60 min prior to beginning ERG.
recumbent and immobilized, it was transferred to a building
Since complete darkness was not possible for the entirety of
within the kangaroo enclosure. Each kangaroo was carefully
the time of dark adaptation due to the need for continued
monitored while under anesthesia, including heart rate and
anesthetic monitoring and the complex intubation process,
rhythm, direct and indirect blood pressure, arterial oxygen
dark adaptation was achieved by using adhesive tape to close
saturation and respiratory rate. After obtaining direct and
the eyelids of each kangaroo and then taping a patch of dark
indirect blood pressure measurements as part of an unre-
material over the eyelids to simulate a dark environment.
lated study, each kangaroo was administered 5% isoflurane
This technique allowed for the necessary pre-ERG dark
(Isoflo; Abbott Animal Health, Abbott Park, IL, USA) by
adaptation without interfering with the work of the
facemask with oxygen at 2–3 L/min. Each kangaroo was
anesthetic team and monitoring. After dark adaptation was
Ó 2010 American College of Veterinary Ophthalmologists, Veterinary Ophthalmology, 13, 41–46
e l e c t r o r e t i n o g r a p h y i n t h e w e s t e r n g r a y k a n g a r o o 4 3
concluded (minimum of 20 min), the ERG was performed
using a monopolar electrode-contact lens (ERG-jet; NicoletInstruments, Madison, WI, USA) applied to the cornea with
hypromellose 2.5% gel as a coupling agent (Gonak; Akorn,Inc., Buffalo Grove, IL, USA), male subdermal platinum
needle electrodes (FD-E2-24; Astro-Medical, Inc. Warwick,RI, USA) and a portable ERG machine, the Handheld
Multispecies ERG (HMsERG) (HMsERG Model 1000;
RetVetCorp, Columbia, MO, USA). The ground electrode
needle was placed at the apex of the occiput directly betweenthe two ears, and the reference needle was placed approxi-
mately 2 cm lateral to the lateral canthus of the eye being
0 10 20 30 40 50 60 70 80 90 100
The Quick Ret Check protocol was used in both eyes
Figure 1. Scatter plot of the 10 mcd.s/m2 ERG b-wave values. At this
of all kangaroos. The Quick Ret Check Protocol, which
low light intensity, no a-wave values are recorded.
is part of the software of the HMsERG unit, was devel-oped by Dr. Kristina Narfstro¨m. The HMsERG unit uti-
lizes a white flash within a mini-Ganzfeld for stimulationof the retina. It utilizes only three levels of light stimuli
All kangaroos had normal ocular examinations at the time of
in order to obtain an overall evaluation of retinal function
ERG. Mean IOP as estimated with applanation tonometry
very quickly with variable flash durations of 0.005–5 ms,
was 12.9 mmHg with SD ± 10.5 mmHg and a range of
depending on the test protocol. The first set consists of
9–20 mmHg. Mean IOP as estimated with rebound tonom-
the average response to four light flashes (2 s in between
etry was 10.1 with SD ± 4.8 mmHg and a range of
flashes) at 10 mcd.s/m2, followed by a single flash at
7–19.5 mmHg. Bilateral ERGs were obtained from all six
3000 mcd.s/m2 and, after 20 s, another single flash at
kangaroos, however in two kangaroos (one male and one
10 000 mcd.s/m2.20 In dark adapted conditions ‘pure’ rod
female), the reading in one eye was uninterpretable. All
responses are obtained through the first set of low light
kangaroos were normotensive, normothermic and neither
intensity flashes, while for the second and third flash
hypoxemic nor hypercapneic at the time of ERG harvesting.
stimuli, the responses are derived from a mixture of rod
At 10 mcd.s/m2 the mean b-wave amplitude and implicit
and cone photoreceptors. The bandpass of the HMsERG
times were 102.0 lV (SD ± 41.3 and 95% CI 68.9–135.1)
and 78.4 ms (SD ± 8.3 and 95% CI 71.8–85.0) (Fig. 1). No
During the ERG, all ambient lights were turned off with
a-wave is obtained in this low amplitude ERG response,
the exception of anesthetic monitoring equipment monitors,
which only consists of a low amplitude and late-onset b-
which remained on but were positioned away from the kan-
wave, for which amplitude and implicit time data is reported.
garoo’s head, and a single 20 watt red light which was used
At 3000 mcd.s/m2 the mean a-wave amplitudes and implicit
to illuminate the kangaroo’s head and the ERG equipment.
times were 69.9 lV (SD ± 20.5 and 95% CI 53.5–86.3) and
Ambient light intensity was not measured. The room in
17.6 ms (SD ± 1.5 and 95% CI 16.4–18.8) and the mean
which all ERGs were performed was not insulated in any
b-wave amplitude and implicit times were 175.4 lV
way from external electrical interference. Both cellular tele-
(SD ± 35.9 and 95% CI 146.7–204.1) and 74.1 ms
phones and laptop computers were present within the exam-
(SD ± 3.5 and 95% CI 71.2–76.9) (Fig. 2). At 10 000 mcd.s/
ination room. At the conclusion of ERG, each kangaroo
m2 the mean a-wave amplitude and implicit times and
received a brief anterior segment examination using diffuse
amplitudes were 89.1 lV (SD ± 27.1 and 95% CI
illumination and indirect funduscopy using a 2.2D condens-
67.5–110.8) and 16.8 ms (SD ± 1.0 and 95% CI 16.0–17.0)
ing hand lens to ensure that no new ophthalmic lesions had
and the mean b-wave amplitude and implicit times were
developed since the previous examination 3 months prior to
203.7 lV (SD ± 41.4 and 95% CI 170.6–236.8) and 75.4 ms
(SD ± 3.3 and 95% CI 72.8–78.1) (Fig. 3). The normal
All ERGs were analyzed using the HMSERG software,
ERG of kangaroo #6 is presented as Fig. 4.
and a-wave and b-wave amplitudes and implicit times wererecorded for each kangaroo. For the four kangaroos in which
bilateral ERGs were obtained the data from the left andright eyes were combined and averaged for a single reading.
This report demonstrates a practical method of performing
The limited data set precluded inferential statistical testing,
ERG on an exotic species. ERG has not previously been
so mean, standard deviation (SD) and 95% confidence inter-
reported in the western gray kangaroo, however one report
val (CI) with alpha = 0.05 were reported for the amplitudes
details the ERG findings and photoreceptor spectral
and implicit times of each ERG (Excel; Microsoft, Inc.,
sensitivities of a related macropod, the tammar wallaby
(Macropus eugenii).21 Veterinary ERG has a wide variety of
Ó 2010 American College of Veterinary Ophthalmologists, Veterinary Ophthalmology, 13, 41–46
Kangaroos as a species are reported to be affected with nutri-tional cataracts, so establishing reference values of normal
ERGs may be of significant diagnostic value.13
Electroretinography is plagued by a myriad of factors that
interfere with accurate and reliable recordings of good qual-ity. Such factors include excessive ambient electrical noise,
inappropriate placement of ground and reference electrodes,
faulty electrodes, poor contact between the corneal surface
and the active electrode, irrelevant physiologic activity andinappropriate or faulty filters and amplifiers.29 In this study,
ERGs were unable to be obtained from one eye of two kan-
0 10 20 30 40 50 60 70 80 90
garoos. Although wide variety of physiologic, pathologic
and pharmacologic factors also influence the ERG, includ-ing body temperature, oxygenation/ventilation status, IOP,
Figure 2. Scatter plot of the 3000 mcd.s/m2 ERG values. The clus-
and sedatives/anesthetics, these parameters were carefully
tered values to the left represent a-wave values while the clustered valuesto the right represent b-wave values.
monitored and are considered unlikely to have contributedto the poor ERG recordings.30 Faulty electrodes and wiringare possible contributors to the poor ERG recordings, how-
ever the electrodes and wiring were successfully utilized for
subsequent recordings, thus making this cause less likely. Excessive external electrical interference was considered a
possible cause of the uninterpretable waveforms, however
the electrical interference within the room (from external
power cords and other electrical equipment) remained con-
stant during the recording period, making this less likely. Amore likely possibility is poor positioning of the reference
electrode, causing amplification of background physiologicnoise or poor contact between the JET electrode and the
0 10 20 30 40 50 60 70 80 90
cornea. A possible improvement of the technique presented
here would be to reposition reference electrodes when poorrecordings were obtained, liberal application of the coupling
Figure 3. Scatter plot of the 10 000 mcd.s/m2 ERG values. The clus-
media between the electrode and the cornea and minimiza-
tered values to the left represent a-wave values while the clustered values
tion of the amount of ambient electrical interference by
to the right represent b-wave values.
turning off unnecessary electrical devices. Future studiesmay investigate alternative corneal electrodes, including a
applications, from the pre-operative screening of patients
microfiber electrode, that may be more appropriate for the
with mature cataracts prior to cataract surgery to complex
curvature and size of the kangaroo cornea.31
diagnostic protocols for detecting subtle changes in rod/
In both human and veterinary ophthalmology, there has
cone function in hereditary retinal degenerations. Although
been a call for standards of uniformity in electrodiagnostic
various research and clinical screening protocols have been
testing of retinal function, an attempt to make results from
well described, there is a paucity of information regarding
different laboratories or clinics more comparable.20,32 The
ERG in exotic species. The size and bulk of most ERG
protocol utilized in the study is modeled after the guidelines
machines have historically limited their field applications
suggested in these consensus statements, however it differs
and use in exotic species that could not be examined in a hos-
from longer and more elaborate protocols in that it is meant
pital setting. With the development of a hand-held ERG
to be a fast screening test and does not give detailed and
machine such as the HMsERG, the feasibility of performing
complete information about rod and cone function sepa-
ERG in exotic species housed in zoological collections has
rately. Cone function tests were not performed in this study
because of time limitations with other phases of the study.
As phacoemulsification in exotic species has become more
The major advantage to the QuickRetCheck protocol used
common, so does the need for accurate and accessible
in this study is its brevity, which is ideal for use under field
ERG.22–28 The purpose of this study was to describe a suc-
research or clinical conditions. The protocol has previously
cessful technique for field ERG in western gray kangaroos,
been utilized in dogs but has not been described in other
however the technique has applications to a wide variety of
species.33 Other possible protocols that could be utilized
exotic species, particularly those for which capture and
that may have the same advantage of brevity include the
transportation to a hospital for pre-operative evaluation is
shorter gross retinal function protocol proposed for use in
either not feasible or not in the best interest of the animal.
Ó 2010 American College of Veterinary Ophthalmologists, Veterinary Ophthalmology, 13, 41–46
e l e c t r o r e t i n o g r a p h y i n t h e w e s t e r n g r a y k a n g a r o o 4 5
Figure 4. Representative recordings using theQuickRetCheck protocol in a 7-year-old westerngray kangaroo. Bilateral recordings are shown withtracings from OS on the left side and tracings fromOD on the right. For evaluation of the rod system(in the dark adapted state) the average of four flashesof low intensity light stimulation (10 cd.s/m2) isused, followed by two single flashes of high intensitylight stimulation, one flash at 3 cd.s/m2 and anotherat 10 cd.s/m2. The latter two light stimuli showresponses of mixed rod and cone photoreceptors.
The role of general anesthesia and its affect on the ERG
described in the western gray kangaroo, however in the
is important for the accurate interpretation of the ERG.
dog, the average duration of action for medetomidine in
Medetomidine is reported to significantly but minimally
the dog is approximately 30 min, and 20 min for keta-
prolong the implicit times and decreases the amplitudes of
mine.37 It is less likely that either ketamine, given its dura-
the canine ERG as evaluated using the HMsERG.33 The
tion of action, or medetomidine, given its duration of
inhalant anesthetic gas isoflurane has been demonstrated
action and the administration of atipamazole as a reversal
to decrease the amplitudes of the a and b-waves compared
agent, significantly impacted the ERG, and therefore
to sedation with tiletamine-zolazepam in normal dark-
isoflurane is likely the largest influence on the ERG out-
adapted dogs, as have the inhalant gasses sevoflurane and
come in this group of anesthetized kangaroos. The implicit
halothane.34,35 The combination of thiopental and isoflura-
times of the b-wave at all light intensities were markedly
ne has been shown to decrease the implicit time and ampli-
increased compared to the identical ERG protocol with
tude of the a wave in normal dogs compared to the
the HMsERG machine in dogs sedated with only mede-
combinations of medetomidine and ketamine or xylazine
tomidine, which may represent a drug effect or normal
and ketamine.36 The anesthesia protocol in this case was
physiology for this exotic species.33 It would be extremely
selected as part of a related study on the affects of two anes-
difficult to perform an ERG in a nonanesthetized adult
thetic protocols on the blood pressure of western gray kan-
kangaroo due to their size and temperament, therefore the
garoos. Medetomidine, an alpha-2-agonist and ketamine, a
results of this study in anesthetized kangaroos provide a
centrally acting N-methyl-D-aspartic acid receptor-inhibi-
reasonable reference range for ERG values at three light
tor, are a commonly used combination for immobilization of
intensities using a field ERG protocol. This study provides
western gray kangaroos. Since medetomidine is reported to
evidence that ERGs can be successfully performed in the
cause peripheral hypertension in dogs, atipamazole was
zoological species using a portable ERG unit and an ERG
administered to the kangaroos in this study after beginning
protocol adapted for field purposes, opening up new
insufflation with isoflurane to eliminate this potentially
avenues for future research in retinal electrophysiology.
confounding affect on measurement of blood pressure. The average time from administration of the ketamine/
medetomidine to the beginning of the ERG was 64.2 minwith a range of 40–83 min. The pharmacokinetics of the
The authors gratefully acknowledge Dr. Hsin-Yi Weng for
anesthetic agents used in this study have not been well
her contribution to the statistical analysis.
Ó 2010 American College of Veterinary Ophthalmologists, Veterinary Ophthalmology, 13, 41–46
20. Marmor MF, Fulton AB, Holder GE et al. ISCEV Standard for
full-field clinical electroretinography (2008 update). Documenta
1. Einthoven W, Jolly W. The form and magnitude of the electrical
response of th eye to stimulation by light at various intensities.
21. Hemmi JM, Maddess T, Mark RF. Spectral sensitivity of
Quarterly Journal of Experimental Physiology 1908; 1: 373–416.
photoreceptors in an Australian marsupial, the tammar wallaby
2. Parry HB. The electroretinogram of the dog. Journal of Physiology
(Macropus eugenii). Vision Research 2000; 40: 591–599.
22. Carter RT, Murphy CJ, Stuhr CM et al. Bilateral phacoemulsifi-
3. Rubin LF. Atrophy of rods and cones in the cat retina. Journal of
cation and intraocular lens implantation in a great horned owl.
the American Veterinary Medical Association 1963; 142: 1415–1420.
Journal of the American Veterinary Medical Association 2007; 230:
4. Gum GG. Electrophysiology in veterinary ophthalmology. Veteri-
nary Clinics of North America. Small Animal Practice 1980; 10:
23. Colitz CM, Lewbart G, Davidson MG. Phacoemulsification in an
adult Savannah monitor lizard. Veterinary Ophthalmology 2002; 5:
5. Miller TR. The uses and limitations of the electroretinogram in
veterinary practice. British Veterinary Journal 1993; 149: 3–4.
24. Cooley PL. Phacoemulsification in a clouded leopard (Neofelis
6. Celesia GG. Anatomy and physiology of visual evoked potentials
nebulosa). Veterinary Ophthalmology 2001; 4: 113–117.
and electroretinograms. Neurologic Clinics 1988; 6: 657–679.
25. Felchle LM, Sigler RL. Phacoemulsification for the management
7. Kofuji P, Ceelen P, Zahs KR et al. Genetic inactivation of an
of Encephalitozoon cuniculi-induced phacoclastic uveitis in a rabbit.
inwardly rectifying potassium channel (Kir4.1 subunit) in mice:
Veterinary Ophthalmology 2002; 5: 211–215.
phenotypic impact in retina. Journal of Neuroscience 2000; 20:
26. Gionfriddo JR. Cataracts in New World camelids (llamas,
alpacas, vicunas, and guanacos). The Veterinary Clinics of North
8. Frishman LJ. Origins of the electroretinogram. In: Principles and
America. Exotic Animal Practice 2002; 5: 357–369.
Practice of Clinical Electrophysiology of Vision, 2nd edn. (eds Hecken-
27. Kelly TR, Walton W, Nadelstein B et al. Phacoemulsification of
lively JR, Arden GB) MIT Press, Cambridge, 2006; 147–174.
bilateral cataracts in a loggerhead sea turtle (Caretta caretta).
9. Durham PJK, Finnie JW, Lawrence DA et al. Blindness in South
Veterinary Record 2005; 156: 774–777.
Australian kangaroos. Australian Veterinary Journal 1996; 73:
28. Wilson D, Pettifer GR. Anesthesia case of the month. Mallard
undergoing phacoemulsification of a cataract. Journal of the
10. Hooper P. Kangaroo blindness and some other new viral diseases
American Veterinary Medical Association 2004; 225: 685–688.
in Australia. Australian Veterinary Journal 1999; 77: 514–515.
29. Komaromy AM, Brooks DE, Dawson WW et al. Technical issues
11. Hooper PT, Lunt RA, Gould AR et al. Epidemic of blindness in
in electrodiagnostic recording. Veterinary Ophthalmology 2002; 5:
kangaroos – evidence of a viral aetiology. Australian Veterinary
30. Ekesten B. Ophthalmic examination and diagnostics Part 4: elect-
12. Schmidt RE, Toft JD. Ophthalmic lesions in animals from a zoo-
rodiagnostic evaluation of vision. In: Veterinary Ophthalmology, 4th
logical collection. Journal of Wildlife Diseases 1981; 17: 267–275.
edn. (ed. Gelatt KN) Blackwell Publishing, Ames, 2007; 1672.
13. Stanley RG. Marsupial ophthalmology. The Veterinary Clinics of
31. Komaromy AM, Andrew SE, Sapp HL Jr et al. Flash electroreti-
North America. Exotic Animal Practice 2002; 5: 371–390.
nography in standing horses using the DTL microfiber electrode.
14. Labelle AL, Low M, Hamor RE, et al. Ophthalmic examination
Veterinary Ophthalmology 2003; 6: 27–33.
findings in a captive mob of western gray kangaroos (Macropus
32. Narfstrom K, Ekesten B, Rosolen SG et al. Guidelines for clinical
fuliginosus). Journal of Zoo and Wildlife Diseases 2010; In press.
electroretinography in the dog. Documenta Ophthalmologica 2002;
15. Kagan RE, Kinsel M, Gloor K et al. Morphologic evidence sug-
gestive of hypertension in western gray kangaroos (Macropus fulig-
33. Norman JC, Narfstrom K, Barrett PM. The effects of medetomi-
inosus). Veterinary Pathology 2009; 46: 977–984.
dine hydrochloride on the electroretinogram of normal dogs.
16. Crispin SM, Mould JR. Systemic hypertensive disease and the
Veterinary Ophthalmology 2008; 11: 299–305.
feline fundus. Veterinary Ophthalmology 2001; 4: 131–140.
34. Lin SL, Shiu WC, Liu PC et al. The effects of different
17. Sicard P, Acar N, Gregoire S et al. Influence of rosuvastatin on
anesthetic agents on short electroretinography protocol in dogs.
the NAD(P)H oxidase activity in the retina and electroretino-
Journal of Veterinary Medical Science 2009; 71: 763–768.
graphic response of spontaneously hypertensive rats. British Jour-
35. Yanase J, Ogawa H. Effects of halothane and sevoflurane on the
nal of Pharmacology 2007; 151: 979–986.
electroretinogram of dogs. American Journal of Veterinary Research
18. Antisedan (Atipamazole). Pfizer Animal Health. Package insert,
36. Jeong MB, Narfstrom K, Park SA et al. Comparison of the effects
19. Tuntivanich N, Mentzer AL, Eifler DM et al. Assessment of the
of three different combinations of general anesthetics on the elec-
dark-adaptation time required for recovery of electroretinographic
troretinogram of dogs. Documenta Ophthalmologica 2009; 119:
responses in dogs after fundus photography and indirect ophthal-
moscopy. American Journal of Veterinary Research 2005; 66:
37. Muir WW, Hubbell JE. Handbook of Veterinary Anesthesia, Mosby,
Ó 2010 American College of Veterinary Ophthalmologists, Veterinary Ophthalmology, 13, 41–46
Advance Access Publication 7 February 2007Juice Powder Concentrate and Systemic Blood Pressure,Progression of Coronary Artery Calcium and AntioxidantStatus in Hypertensive Subjects: A Pilot StudyM. C. Houston1, B. Cooil2, B. J. Olafsson3 and P. Raggi41Hypertension Institute of Nashville, Vanderbilt University School of Medicine and Saint Thomas Hospital,2Owen Graduate School of Management, Vand
Jahresbericht 2008 Abteilung f. Psychiatrie/ Psychiatrie I Leiter : Sekretariat : 1. Personalbesetzung zum 31.12.2008 Fachärzte : Assistenzärzte : Dr. Barbara Plattner Dr. Bettina Schletterer Dr. Susanne Schuler Turnusärzte : Abteilungsschwester : Osr. Andrea Reinthaler 2. Bericht: Wie bereits in den letzten Jahresberichten festgestellt, besch�

 e l e c t r o r e t i n o g r a p h y i n t h e w e s t e r n g r a y k a n g a r o o 4 3
concluded (minimum of 20 min), the ERG was performed
using a monopolar electrode-contact lens (ERG-jet; NicoletInstruments, Madison, WI, USA) applied to the cornea with
hypromellose 2.5% gel as a coupling agent (Gonak; Akorn,Inc., Buffalo Grove, IL, USA), male subdermal platinum
needle electrodes (FD-E2-24; Astro-Medical, Inc. Warwick,RI, USA) and a portable ERG machine, the Handheld
Multispecies ERG (HMsERG) (HMsERG Model 1000;
RetVetCorp, Columbia, MO, USA). The ground electrode
needle was placed at the apex of the occiput directly betweenthe two ears, and the reference needle was placed approxi-
mately 2 cm lateral to the lateral canthus of the eye being
0 10 20 30 40 50 60 70 80 90 100
e l e c t r o r e t i n o g r a p h y i n t h e w e s t e r n g r a y k a n g a r o o 4 3
concluded (minimum of 20 min), the ERG was performed
using a monopolar electrode-contact lens (ERG-jet; NicoletInstruments, Madison, WI, USA) applied to the cornea with
hypromellose 2.5% gel as a coupling agent (Gonak; Akorn,Inc., Buffalo Grove, IL, USA), male subdermal platinum
needle electrodes (FD-E2-24; Astro-Medical, Inc. Warwick,RI, USA) and a portable ERG machine, the Handheld
Multispecies ERG (HMsERG) (HMsERG Model 1000;
RetVetCorp, Columbia, MO, USA). The ground electrode
needle was placed at the apex of the occiput directly betweenthe two ears, and the reference needle was placed approxi-
mately 2 cm lateral to the lateral canthus of the eye being
0 10 20 30 40 50 60 70 80 90 100


 Kangaroos as a species are reported to be affected with nutri-tional cataracts, so establishing reference values of normal
ERGs may be of significant diagnostic value.13
Electroretinography is plagued by a myriad of factors that
interfere with accurate and reliable recordings of good qual-ity. Such factors include excessive ambient electrical noise,
inappropriate placement of ground and reference electrodes,
faulty electrodes, poor contact between the corneal surface
and the active electrode, irrelevant physiologic activity andinappropriate or faulty filters and amplifiers.29 In this study,
ERGs were unable to be obtained from one eye of two kan-
0 10 20 30 40 50 60 70 80 90
Kangaroos as a species are reported to be affected with nutri-tional cataracts, so establishing reference values of normal
ERGs may be of significant diagnostic value.13
Electroretinography is plagued by a myriad of factors that
interfere with accurate and reliable recordings of good qual-ity. Such factors include excessive ambient electrical noise,
inappropriate placement of ground and reference electrodes,
faulty electrodes, poor contact between the corneal surface
and the active electrode, irrelevant physiologic activity andinappropriate or faulty filters and amplifiers.29 In this study,
ERGs were unable to be obtained from one eye of two kan-
0 10 20 30 40 50 60 70 80 90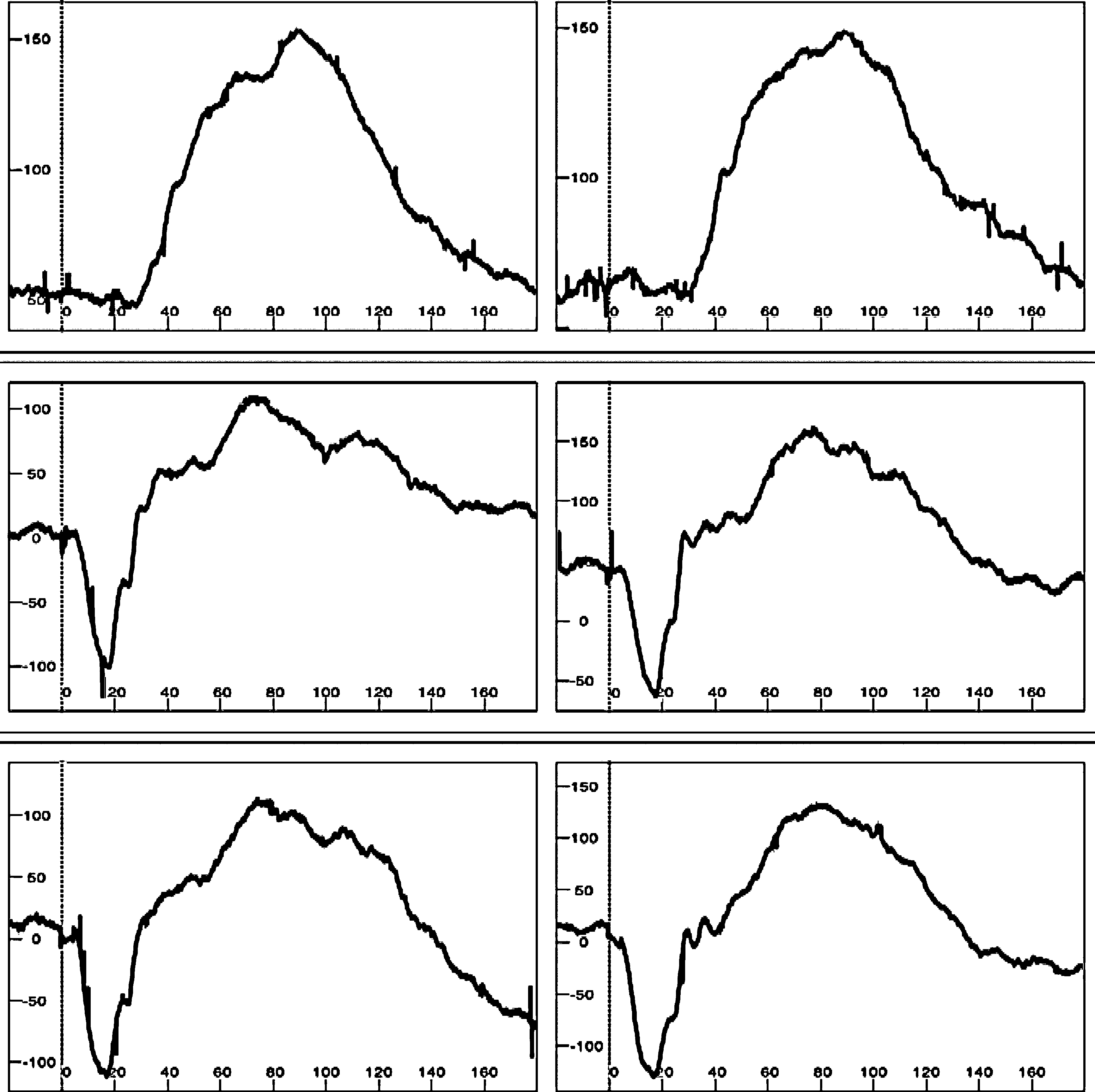 e l e c t r o r e t i n o g r a p h y i n t h e w e s t e r n g r a y k a n g a r o o 4 5
Figure 4. Representative recordings using theQuickRetCheck protocol in a 7-year-old westerngray kangaroo. Bilateral recordings are shown withtracings from OS on the left side and tracings fromOD on the right. For evaluation of the rod system(in the dark adapted state) the average of four flashesof low intensity light stimulation (10 cd.s/m2) isused, followed by two single flashes of high intensitylight stimulation, one flash at 3 cd.s/m2 and anotherat 10 cd.s/m2. The latter two light stimuli showresponses of mixed rod and cone photoreceptors.
e l e c t r o r e t i n o g r a p h y i n t h e w e s t e r n g r a y k a n g a r o o 4 5
Figure 4. Representative recordings using theQuickRetCheck protocol in a 7-year-old westerngray kangaroo. Bilateral recordings are shown withtracings from OS on the left side and tracings fromOD on the right. For evaluation of the rod system(in the dark adapted state) the average of four flashesof low intensity light stimulation (10 cd.s/m2) isused, followed by two single flashes of high intensitylight stimulation, one flash at 3 cd.s/m2 and anotherat 10 cd.s/m2. The latter two light stimuli showresponses of mixed rod and cone photoreceptors.