La spécificité du tadalafil est liée à sa longue demi-vie, permettant une action qui excède largement celle des autres inhibiteurs de PDE5. L’absorption digestive est complète, avec un pic plasmatique atteint en 2 heures environ. Le métabolisme est réalisé via CYP3A4, produisant des métabolites inactifs éliminés principalement dans les fèces. La sélectivité enzymatique est élevée, réduisant les effets indésirables extra-caverneux. Les réactions indésirables fréquentes incluent céphalées, bouffées vasomotrices et troubles digestifs légers. L’activité pharmacologique est stable, indépendamment de l’ingestion d’aliments. Dans les comparaisons de longue durée, acheter cialis pas cher est mentionné en relation avec les études portant sur la persistance d’efficacité et la constance de la cinétique plasmatique.
Doi:10.1016/j.ijgo.2005.10.00
International Journal of Gynecology and Obstetrics (2006) 92, 10 — 18
Misoprostol in preventing postpartum hemorrhage:A meta-analysis
Epidemiology and Biostatistics, School of Public Health, University of California at Berkeley,Berkeley, CA, USA
Received 25 May 2005; received in revised form 3 October 2005; accepted 4 October 2005
Objective: To assess misoprostol’s ability to prevent postpartum hemorrhage
(PPH) where no alternatives exist. Comparison to oxytocics demonstrates how
similarly misoprostol achieves a level of effectiveness—obtainable only in
hospitals—in remote locations around the world. Method: Using the Mantel—
Haenszel fixed-effects model and the DerSirmonian and Laird random-effects
model, summary statistics indicated that misoprostol’s excess risk of PPH was only4% when compared to oxytocics. Result: This risk difference was well within therange of expected results for all uterotonic agents and does not warrant brandingmisoprostol as an inferior drug. Conclusion: Conventional uterotonic drugs shouldnot be used to set the lowest-accepted level of effectiveness in settings wherethey are entirely unsuitable. Continuing to weigh the benefits of one effectivedrug against another only delays the distribution of misoprostol in countries whereit is the only feasible choice and must be measured against no treatment at all. D 2005 International Federation of Gynecology and Obstetrics. Published by ElsevierIreland Ltd. All rights reserved.
quarter of these deaths . Most of these deathsoccur in the resource-poor countries of Africa and
The World Health Organization (WHO) estimated that
Asia, particularly in rural areas. Not surprisingly,
529,000 women died from obstetric causes in 2000
records of maternal mortality are poor or non-
. Postpartum hemorrhage (PPH), which afflicts
existent where it most often occurs, which implies
approximately 14 million women annually, caused a
that even these sobering estimates are greatlyunderestimated. Indeed, data in remote regions areso scarce and the methods of collection so varied thatthe WHO warns against the formulation of confidence
E-mail address: [email protected].
intervals around the available estimates.
0020-7292/$ - see front matter D 2005 International Federation of Gynecology and Obstetrics. Published by Elsevier Ireland Ltd. All rights reserved. doi:10.1016/j.ijgo.2005.10.001
Misoprostol in preventing postpartum hemorrhage: A meta-analysis
PPH is defined as blood loss of 500 mL or more
developing countries, where it is most needed.
within 24 h of delivery, but, this quantity is
Misoprostol’s value as a prophylactic uterotonic
extremely difficult to identify outside of a con-
drug lies in its ability to prevent PPH and reduce
trolled trial setting. Even trained physicians are
maternal mortality where no alternatives exist.
reported to typically underestimate blood loss by
Comparison to oxytocics should serve only to
about half While there are a few known risk
demonstrate how similarly misoprostol achieves a
factors, PPH occurrence is random, making it
level of effectiveness—obtainable only in hospi-
impossible to predict in both low and high risk
tals—in remote locations around the world. To
populations. Furthermore, blood loss can be rapid.
date, this is the largest meta-analysis ever con-
In developing countries, where nearly half the
ducted on the efficacy of misoprostol for the
women deliver without the aid of a skilled birth
attendant , there is simply not enough time toseek treatment for PPH, and in most cases none isto be had. The only way to help women without
access to trained attendants is through preventa-tive measures.
A literature search was conducted for all random-
The most successful method for reducing PPH,
ized control trials (RCT) which tested misoprostol’s
Active Management of the Third Stage of Labor
efficacy in preventing PPH. The electronic data-
(AMTSL), requires prophylactic uterotonic drugs
base PubMed (National Library of Medicine,
which are unsuitable for use in the remote loca-
Bethesda, MD) was searched for published articles,
tions where prevention is most needed. Nonethe-
along with the Cochrane CENTRAL database and the
less, this nearly universal method has set the
Population Council’s bibliographic website
precedent for a standard of care unavailable in
developing countries. The uterotonic drugs used in
ing terms used were: misoprostol and postpartum
AMTSL trials include oxytocics: oxytocin (Syn-
hemorrhage, coupled with: prevention and active
tocinonR, Alliance Pharmaceuticals, Chippenham,
management. References from published articles
UK or PitocinR, King Pharmaceuticals, Bristol, TN),
were pursued and primary authors contacted in
ergometrine malate (MethergineR, Novartis Phar-
order to uncover any unpublished RCTs. The search
maceuticals, East Hanover, NJ) and combinations of
was conducted irrespective of language of publica-
the two (SyntometrineR, Alliance Pharmaceuticals,
tion or geographic region. All studies matching the
Chippenham, UK) all of which must be administered
inclusion criteria and published before May 2005
by injection, which not only requires a sterile
needle, syringe and accurate dosing, but someoneto administer it. In addition, oxytocics are light-sensitive and require refrigeration to remain phar-macologically active, which limits their use to areas
with refrigeration and reliable sources of energyand increases their cost.
All RCTs which assessed misoprostol efficacy in
Misoprostol (CytotecR, Pfizer, New York, NY), a
preventing PPH during third trimester vaginal births
prostaglandin E1 analog, registered for the pre-
were reviewed for inclusion in this analysis. All
vention and treatment of gastric ulcers, is well-
studies, irrespective of dose, route of administra-
known for its off-label use as a uterotonic agent. It
tion (with the exception of vaginal administration
is inexpensive (one 200 g tablet is approximately
due to its infeasibility after a vaginal birth) or type
US$1 comes in tablets which can be admin-
of control substance, were included. Three out-
istered orally, rectally or sublingually, and does not
comes were selected before analysis began: blood
require refrigeration, dark storage or administra-
loss z500 mL, blood loss z1000 mL and the need
tion by an attendant. However, many studies have
for additional uterotonic agents. Because the side
found it to be slightly less effective than oxytocics
effects of all uterotonic drugs have been well
in controlled clinical settings. This circumstance
has had the result of branding misoprostol as an
ison to the life threatening alternative of PPH, side
inferior drug , despite repeated praise for
effects were not considered a relevant outcome for
the feasibility of its use in resource-poor settings
A total of 31 relevant studies were identified,
The objective of this review is to analyze all
but only 22 were selected for inclusion in the meta-
existing trial data in order to reframe the current
analysis. Six studies were excluded due to miso-
debate surrounding the use of misoprostol in
prostol being administered vaginally or after
.5 mg or Oxytocin 10 units orErgometrine 500 mg
a New studies since last meta-analysis.
Misoprostol in preventing postpartum hemorrhage: A meta-analysis
All doses and routes of administration were
pooled for three reasons. First, patients within
studies were already included in other trials
individual studies did not always receive the same
and could not be used independently. A final trial
was eliminated because it reported a pilot study
it impossible to distinguish between methods.
Although the pooling of patients given oxytocics
The studies which were included consisted of
of varying administrations has been heavily criti-
five placebo-controlled trials and 26 drug
cized, especially in the WHO multi-center trial
where intravenous and intramuscular administra-
but in two instances , where three different
heterogeneity only strengthened this meta-analy-
oxytocics were tested, two arms were excluded
sis. As oral, rectal and sublingual routes are known
from the meta-analysis since they could not be
to have slower up-take than intravenous or intra-
pooled and analyzed against the misoprostol arm
muscular injections, testing the three slowest
simultaneously. For these two trials, the oxytocin
methods against the two fastest biased the results
arm was selected for the analysis since it is the
against finding a similar relative risk. Therefore,
most common prophylactic uterotonic drug. Seven
the difference between misoprostol and oxytocics
found in this analysis was actually greater than if
published subsequent to the only other meta-
misoprostol had only been administered by its
analysis on the efficacy of misoprostol, published
fastest method (sublingual and oxytocics by
their slowest (intramuscularly). Second, numerousstudies on the efficacy of different oxytocics foundno significantly statistical difference in blood lossbetween them And third, comparison of
misoprostol to each of these individual drugs hasalready been well documented ; given these
Data were extracted from each study by the author,
caveats, the purpose of this analysis was to
who was not blinded. A validity analysis was
compare misoprostol to the de facto standard of
conducted to assess the methodological aspects of
care (i.e. the collective efficacy of any drug
each trial. Studies were scored from 0 to 10, using a
approved for PPH prevention), rather than any
For each outcome, a pooled risk ratio (RR) was
1) A research objective appropriate for this
calculated comparing misoprostol to oxytocics or
placebo. The Mantel—Haenszel fixed-effects model
2) Explicit inclusion and exclusion criteria
was used instead of the inverse-variance method
3) Exclusion of patients with labor augmentation
due to sparse outcome data. The test for hetero-
geneity was based on weights provided by the
inverse-variance method. When heterogeneity was
5) Reported baseline similarity between groups
detected, the DerSirmonian and Laird random-
effects model was used. Sensitivity analyses were
conducted to investigate the influence of individual
studies on the summary statistic by omitting each
9) No losses to follow-up before each outcome
study in turn. Egger’s weighted regression and
Begg’s rank correlation, where odds ratios were
10) Criteria for administration of additional ute-
plotted against study size, were used for the
detection of publication bias for each outcome.
Analysis of the data was performed using STATA
8.0 statistical software package (STATA Corpora-
tion, College Station, TX). The raw data publishedin each article were compiled in two-by-two tables.
A total of 30,017 participants were included in the
For only one study was it necessary to calculate cell
22 studies in the analysis, approximately half of
counts from the reported percentages How-
whom received misoprostol, with the remainder
ever, not every study reported data for each
specified outcome. When no data were provided,
However, in several instances when the studies
the study was dropped from the model.
reported a loss to follow-up for a specific outcome
a One included study only reported outcome measurements for 500 mL.
misoprostol to placebo (n = 1706) produced a RR of
the available data, not the original sample size, to
0.69 (95% CI: 0.53, 0.90). Thus, at this level
avoid the inherent presumption that those lost to
misoprostol demonstrates clear and statistically
follow-up were not cases. Due to the infrequent
significant reduction in the need for therapeutic
incidence of PPH, little difference was found
between the odds ratios (OR) and RR for any
The 15 studies (n = 26,870) comparing misopros-
tol and oxytocics for blood loss N500 mL produced a
Whereas five studies compared misoprostol and
RR of 1.4, which represents an excess risk (or risk
placebo use, only two reported blood loss N500 mL;
difference) of 5% greater incidence of blood loss
thus, no analysis was conducted for this outcome
level. Pooling the four studies reporting blood loss
studies, a comparison of the fixed effects estimate
N 1000 mL and one which only reported blood loss of
and the random effects estimate showed little
N 500 mL (n = 2112), misoprostol’s risk of
difference between the two models. Although it
PPH incidence over the risk of incidence with
initially appeared that the largest trial dom-
placebo was 0.85 (RR). Although misoprostol
inated the pooled estimates, removing this study
appeared to decrease the risk of PPH, this finding
did not significantly alter the results (RR: 1.39; 95%
was not statistically significant (95% CI: 0.63, 1.14).
CI: 1.219, 1.588). Further sensitivity analyses
One included study specifically stated that its
demonstrated that the heterogeneity present in
objective was to measure side effects and was
these models was the effect of the 15 varied
not intended to be an efficacy trial due to its lack
outcomes, not the effect of any single study.
of statistical power , which could help explain
The RR of 1.36 for the 11 studies reporting blood
this lack of significance. Of interest, including that
loss N1000 mL for misoprostol versus oxytocics
study with the three other trials reporting a need
(n = 25,448) only demonstrated a 1% excess risk of
for additional uterotonic agents when comparing
All studies evaluating misoprostol vs. placebo with outcome blood loss N1000 mL. Mantel—Haenszel fixed-
effects model. Heterogeneity chi-squared = 4.09 (df = 4), p = 0.394. I-squared (variation in RR attributable toheterogeneity) = 2.1%. Test of RR = 1: z = 1.08, p = 0.280. **Estimate reported for 500 mL or greater.
Misoprostol in preventing postpartum hemorrhage: A meta-analysis
All studies evaluating misoprostol vs. placebo with outcome of additional uterotonic agents. Mantel—
Haenszel fixed-effects model. Heterogeneity chi-squared = 1.62 (df = 3), p = 0.654. I-squared (variation in RRattributable to heterogeneity) = 0.0%. Test of RR = 1: z = 2.71, p = 0.007.
from this model produced a statistically insignifi-
many milliliters lost warranted further interven-
cant summary estimate (RR: 1.25; 95% CI: 0.94,
tion. Because rectal administration of misoprostol
0.167), however this outcome was found to be
requires a longer time to reach peak concentration
consistent with the other studies’ findings and was
levels than oral misoprostol it is possible that
many studies intervened with additional uterotonic
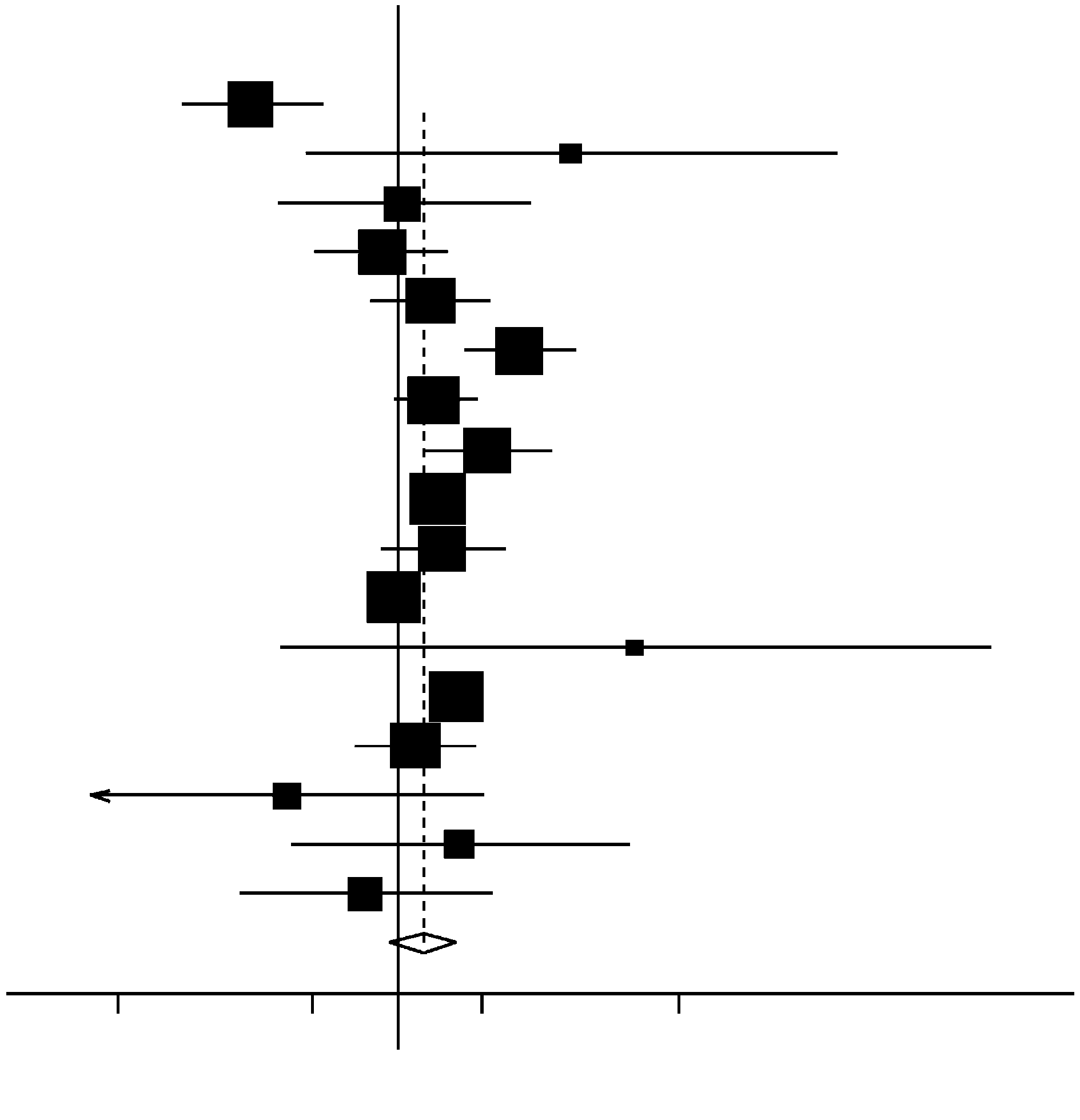
The random effects model of the 17 studies
agents before there was adequate time for the
comparing the need for additional uterotonic drugs
misoprostol to take effect. A sub-analysis of oral
in patients who received prophylactic misoprostol
and sublingual misoprostol revealed no statistical
to patients receiving oxytocics (n = 27,566) pro-
difference between misoprostol and oxytocics (RR:
duced a summary RR of 1.23 ). The hetero-
1.13, 95% CI: 0.81, 1.56). This observation strongly
geneity present in this model can, in large part, be
suggests that the rectal misoprostol had, in fact,
explained by the subjective point at which addi-
not yet peaked when additional uterotonic agents
tional uterotonic drugs were administered. Not
were administered. Therefore, inclusion of rectally
only did many studies estimate (as opposed to
administered misoprostol only masked the equiva-
measure) blood loss, but not one specified how
lency of oral and sublingual misoprostol to oxy-
All studies evaluating misoprostol vs. oxytocics with outcome blood loss N500 mL
95% CI = 95% Confidence intervals. M—H pooled RR = Mantel—Haenszel pooled risk ratios.
All studies evaluating misoprostol vs. oxytocics with outcome blood loss N1000 mL. Mantel—Haenszel fixed-
effects model. Heterogeneity chi-squared = 3.64 (df = 10), p = 0.962. I-squared (variation in RR attributable toheterogeneity) = 0.0%. Test of RR = 1: z = 4.41, p = 0.000.
tocics. Despite many misoprostol patients receiving
occurs in 5—18% of live births many trial
doses which had not fully taken effect, only 4%
findings were not statistically significant. The wide
more received therapeutic drugs than patients in
confidence intervals reflected the high probability
of chance in each of these trials. Therefore, the RRof each trial were not definitive estimates, as itwas impossible to distinguish between individual RR
with overlapping confidence intervals. However,the fact that the RR were consistent with individual
Due to the small sample sizes and PPH’s high
studies’ findings, demonstrated that the overall
variability in general (even with oxytocics PPH
risk of PPH when misoprostol was used was only 4%
All studies evaluating misoprostol vs. oxytocics with outcome of additional uterotonic agents. DerSirmonian
and Laird random-effects model. Heterogeneity chi-squared = 343.00 (df = 16), p = 0.000. I-squared (variation in RRattributable to heterogeneity) = 95.3%. Estimate of between-study variance Tau-squared = 0.2171. Test of RR = 1:z = 1.47, p = 0.141.
Misoprostol in preventing postpartum hemorrhage: A meta-analysis
greater than when oxytocics were used. This risk
[5] Roman AS, Andrei R. Seven ways to control postpartum
difference was well within the range of expected
hemorrhage. Contemp OB/GYN 2003;3:34 – 53.
[6] Chong YS, Su LL, Arulkumaran S. Current strategies for the
results for any uterotonic agent and was not
prevention of postpartum haemorrhage in the third stage of
unique to misoprostol. Not surprisingly, the meta-
labour. Curr Opin Obstet Gynecol 2004;16(2):143 – 50.
analysis published in 2003 had similar findings.
[7] Villar J, Gulmezoglu AM, Hofmeyr GJ, Forna F. Systematic
In that review, Joy et al. reported OR for misopros-
review of randomized controlled trials of misoprostol to
tol versus oxytocin of 1.51 at blood loss
prevent postpartum hemorrhage. Obstet Gynecol 2002;
and 2.14 for additional oxytocics needed. Stated
[8] Mousa HA, Walkinshaw S. Major postpartum haemorrhage.
another way, these OR only represented an excess
Curr Opin Obstet Gynecol 2001;13(6):595 – 603.
risk of 5.8% and 4.5%, respectively. Although the
[9] Darney PD. Misoprostol: a boon to safe motherhood or not?
report stated that misoprostol was binferiorQ to
other uterotonic drugs, its value in developing
[10] El-Refaey H, Rodeck C. Post-partum haemorrhage: defini-
tions, medical and surgical management. A time for
countries was not dismissed due to its efficacy over
change. Br Med Bull 2003;67:205 – 17.
[11] Joy SD, Sanchez-Ramos L, Kaunitz AM. Misoprostol use
The primary limitation of this meta-analysis was
during the third stage of labor. Int J Gynaecol Obstet
the inability to conduct sub-analyses due to the
small number of studies using each dose, adminis-
[12] Miller S, Lester F, Hensleigh P. Prevention and treatment of
postpartum hemorrhage: new advances for low-resource
tration and uterotonic drug. Potential systematic
settings. J Midwifery Women’s Health 2004;49(4):283 – 92.
biases, mentioned previously, were the inconsisten-
[13] Potts M, Campbell M. Three meetings and fewer funerals—
cy in blood loss measurement and lack of double-
misoprostol in postpartum haemorrhage. Lancet 2004;
masking. Because all outcomes were dependent on
the amount of blood lost, it was critical to have
[14] McCormick ML, Sanghvi HC, Kinzie B, McIntosh N. Prevent-
ing postpartum hemorrhage in low-resource settings. Int J
uniform measurement across, as well as within,
Gynaecol Obstet 2002;77(3):267 – 75.
studies. Furthermore, because determining the
[15] Hofmeyr GJ, Walraven G, Gulmezoglu AM, Maholwana B,
severity of blood loss requires subjective judgment,
Alfirevic Z, Villar J. Misoprostol to treat postpartum
having all trial investigators and attending physi-
haemorrhage: a systematic review. BJOG 2005;112(5):
cians masked to drug allocation was exceedingly
[16] Diaz QR, Arechiga EM, Resendiz BV, Lopez CO, Ayup HS,
important. For these reasons, both double-masking
Cuervo MJ. Vaginal misoprostol in the prevention of post-
and blood measurement were criteria for the
partum hemorrhage. Ginecol Obstet Mex 2002;70:572 – 5.
validity test. The tests for publication bias showed
[17] Acharya G, Al-Sammarai MT, Patel N, Al-Habib A, Kiserud T.
no strong evidence of bias for any outcome level.
A randomized, controlled trial comparing effect of oral
Nonetheless, there was a surprising lack of placebo
misoprostol and intravenous syntocinon on intra-operativeblood loss during cesarean section. Acta Obstet Gynecol
trials, despite nearly every study concluding with a
request for more trials of this nature.
[18] Lokugamage AU, Paine M, Bassaw-Balroop K, Sullivan KR,
Conventional uterotonic drugs, limited in their
Refaey HE, Rodeck CH. Active management of the third
use in remote areas, should not be used to set the
stage at caesarean section: a randomised controlled trial of
lowest-accepted standard for situations where they
misoprostol versus syntocinon. Aust N Z J Obstet Gynaecol2001;41(4):411 – 4.
are entirely unsuitable. Continuing to weigh the
[19] Chong YS, Chua S, El-Refaey H, Choo WL, Chanrachakul B,
benefits of one effective drug against another,
Tai BC, et al. Postpartum intrauterine pressure studies of
when only misoprostol is currently feasible in
the uterotonic effect of oral misoprostol and intramuscular
developing countries, only delays its necessary
syntometrine. BJOG 2001;108(1):41 – 7.
[20] Diab KM, Ramy AR, Yehia MA. The use of rectal misoprostol
as active pharmacological management of the third stage oflabor. J Obstet Gynaecol Res 1999;25(5):327 – 32.
[21] El-Refaey H, O’Brien P, Morafa W, Walder J, Rodeck C. Use
of oral misoprostol in the prevention of postpartumhaemorrhage. Br J Obstet Gynaecol 1997;104(3):336 – 9.
[1] Maternal Mortality in 2000: estimates developed by WHO,
[22] Lumbiganon P, Villar J, Piaggio G, Gulmezoglu AM, Adetoro L,
UNICEF and UNFPA. Geneva7 The World Health Organiza-
Carroli G. Side effects of oral misoprostol during the first 24
hours after administration in the third stage of labour. BJOG
[2] Mother—baby package: implementing safe motherhood in
countries, vol. 94. Geneva7 World Health Organization,
[23] Wright JM, Newton W. Is rectal misoprostol as effective as
oxytocin in preventing postpartum hemorrhage? J Fam
[3] Tsu VD, Langer A, Aldrich T. Postpartum hemorrhage in
developing countries: is the public health community using
[24] Lumbiganon P, Hofmeyr J, Gulmezoglu AM, Pinol A, Villar J.
the right tools? Int J Gynaecol Obstet 2004;85(Suppl 1):
Misoprostol dose-related shivering and pyrexia in the third
stage of labour. WHO Collaborative Trial of Misoprostol in
[4] Coverage of Maternity Care: a listing of available informa-
the Management of the Third Stage of Labour. Br J Obstet
tion. Fourth edn. Geneva7 World Health Organization; 1997.
[25] Bamigboye AA, Hofmeyr GJ, Merrell DA. Rectal misopros-
rhage after vaginal delivery. Am J Obstet Gynecol
tol in the prevention of postpartum hemorrhage: a
placebo-controlled trial. Am J Obstet Gynecol 1998;
[38] Gulmezoglu AM, Villar J, Ngoc NT, Piaggio G, Carroli G,
Adetoro L, et al. WHO multicentre randomised trial of
[26] Benchimol M, Gondry J, Mention JE, Gagneur O, Boulanger
misoprostol in the management of the third stage of labour.
JC. Role of misoprostol in the delivery outcome. J Gynecol
Obstet Biol Reprod (Paris) 2001;30(6):576 – 83.
[39] Karkanis SG, Caloia D, Salenieks ME, Kingdom J, Walker M,
[27] Hofmeyr GJ, Nikodem VC, de Jager M, Drakely A. Side-
Meffe F, et al. Randomized controlled trial of rectal
effects of oral misoprostol in the third stage of labour—a
misoprostol versus oxytocin in third stage management. J
randomised placebo-controlled trial. S Afr Med J 2001;
Obstet Gynaecol Can 2002;24(2):149 – 54.
[40] Kundodyiwa TW, Majoko F, Rusakaniko S. Misoprostol versus
[28] Hofmeyr GJ, Nikodem VC, de Jager M, Gelbart BR. A
oxytocin in the third stage of labor. Int J Gynaecol Obstet
randomised placebo controlled trial of oral misoprostol in
the third stage of labour. Br J Obstet Gynaecol 1998;
[41] Lam H, Tang OS, Lee CP, Ho PC. A pilot-randomized
comparison of sublingual misoprostol with syntometrine
[29] Surbek DV, Fehr PM, Hosli I, Holzgreve W. Oral misoprostol
on the blood loss in third stage of labor. Acta Obstet
for third stage of labor: a randomized placebo-controlled
Gynecol Scand 2004;83(7):647 – 50.
trial. Obstet Gynecol 1999;94(2):255 – 8.
[42] Oboro VO, Tabowei TO. A randomised controlled trial of
[30] Amant F, Spitz B, Timmerman D, Corremans A, Van Assche
misoprostol versus oxytocin in the active management of
FA. Misoprostol compared with methylergometrine for the
the third stage of labour. J Obstet Gynaecol 2003;23(1):
prevention of postpartum haemorrhage: a double-blind
randomised trial. Br J Obstet Gynaecol 1999;106(10):
[43] Ray A, Mukherjee P, Basu G, Chatterjee A. Misoprostol and
third stage of labour. J Obstet Gynecol Ind 2001 (Novem-
[31] Bamigboye AA, Merrell DA, Hofmeyr GJ, Mitchell R.
Randomized comparison of rectal misoprostol with Synto-
[44] Vimala N, Mittal S, Kumar S, Dadhwal V, Mehta S. Sublingual
metrine for management of third stage of labor. Acta
misoprostol versus methylergometrine for active manage-
Obstet Gynecol Scand 1998;77(2):178 – 81.
ment of the third stage of labor. Int J Gynaecol Obstet
[32] Bugalho A, Daniel A, Faundes A, Cunha M. Misoprostol for
prevention of postpartum hemorrhage. Int J Gynaecol
[45] Walley RL, Wilson JB, Crane JM, Matthews K, Sawyer E,
Hutchens D. A double-blind placebo controlled randomised
[33] Caliskan E, Dilbaz B, Meydanli MM, Ozturk N, Narin MA,
trial of misoprostol and oxytocin in the management of the
Haberal A. Oral misoprostol for the third stage of labor: a
third stage of labour. BJOG 2000;107(9):1111 – 5.
randomized controlled trial. Obstet Gynecol 2003;101(5 Pt
[46] Jadad A. Randomized control trials. London7 BMJ Books;
[34] Caliskan E, Meydanli MM, Dilbaz B, Aykan B, Sonmezer M,
[47] El-ReFaey H. Use of misoprostol in third stage of labour.
Haberal A. Is rectal misoprostol really effective in the
Lancet 2002;359(9307):707 – 8 [discussion 709—710].
treatment of third stage of labor? A randomized controlled
[48] El-Refaey H, O’Brien P, Morafa W, Walder J, Rodeck C.
trial. Am J Obstet Gynecol 2002;187(4):1038 – 45.
Misoprostol for third stage of labour. Lancet 1996;
[35] Cook CM, Spurrett B, Murray H. A randomized clinical trial
comparing oral misoprostol with synthetic oxytocin or
[49] Khan R, Sharma S. Use of misoprostol in third stage of labour.
syntometrine in the third stage of labour. Aust N Z J Obstet
Lancet 2002;359(9307):708 – 9 [author reply 709—710].
[50] O’Brien P, Lokugamage AU, Guillebaud J, Rodeck CH. Use of
[36] El-Refaey H, Nooh R, O’Brien P, Abdalla M, Geary M, Walder
misoprostol in third stage of labour. Lancet 2002;
J, et al. The misoprostol third stage of labour study: a
359(9307):708 [author reply 709—710].
randomised controlled comparison between orally admin-
[51] Shannon C, Winikoff B. Use of misoprostol in third stage of
istered misoprostol and standard management. BJOG
labour. Lancet 2002;359(9307):709 [author reply 709—710].
[52] McDonald S, WJP, DE. Prophylactic syntometrine vs. oxyto-
[37] Gerstenfeld TS, Wing DA. Rectal misoprostol versus intra-
cin in the third stage of labour. The Cochrane Library; 1998.
venous oxytocin for the prevention of postpartum hemor-
Surveillance and Response to Prevent Malaria Re-emergence Alexandre Macedo de Oliveira, MD, MSc, PhD Division of Parasitic Diseases and Malaria Centers for Disease Control and Prevention • Discuss thoughts about malaria reemergence (thoughts, due to limited information on the topic) • Discuss interventions to prevent and/or respond to such events • K
CURRICULUM VITAE INFORMAZIONI PERSONALI Data di nascita Qualifica Amministrazione Incarico attuale Numero telefonico dell’ufficio Fax dell’ufficio E-mail istituzionale TITOLI DI STUDIO E PROFESSIONALI ED ESPERIENZE LAVORATIVE Titolo di studio Altri titoli di studio e professionali Dottorato di Ricerca in Neuroscienze, Perfezionamentopresso la Cla
 International Journal of Gynecology and Obstetrics (2006) 92, 10 — 18
Misoprostol in preventing postpartum hemorrhage:A meta-analysis
Epidemiology and Biostatistics, School of Public Health, University of California at Berkeley,Berkeley, CA, USA
Received 25 May 2005; received in revised form 3 October 2005; accepted 4 October 2005
Objective: To assess misoprostol’s ability to prevent postpartum hemorrhage
(PPH) where no alternatives exist. Comparison to oxytocics demonstrates how
similarly misoprostol achieves a level of effectiveness—obtainable only in
hospitals—in remote locations around the world. Method: Using the Mantel—
Haenszel fixed-effects model and the DerSirmonian and Laird random-effects
model, summary statistics indicated that misoprostol’s excess risk of PPH was only4% when compared to oxytocics. Result: This risk difference was well within therange of expected results for all uterotonic agents and does not warrant brandingmisoprostol as an inferior drug. Conclusion: Conventional uterotonic drugs shouldnot be used to set the lowest-accepted level of effectiveness in settings wherethey are entirely unsuitable. Continuing to weigh the benefits of one effectivedrug against another only delays the distribution of misoprostol in countries whereit is the only feasible choice and must be measured against no treatment at all.
International Journal of Gynecology and Obstetrics (2006) 92, 10 — 18
Misoprostol in preventing postpartum hemorrhage:A meta-analysis
Epidemiology and Biostatistics, School of Public Health, University of California at Berkeley,Berkeley, CA, USA
Received 25 May 2005; received in revised form 3 October 2005; accepted 4 October 2005
Objective: To assess misoprostol’s ability to prevent postpartum hemorrhage
(PPH) where no alternatives exist. Comparison to oxytocics demonstrates how
similarly misoprostol achieves a level of effectiveness—obtainable only in
hospitals—in remote locations around the world. Method: Using the Mantel—
Haenszel fixed-effects model and the DerSirmonian and Laird random-effects
model, summary statistics indicated that misoprostol’s excess risk of PPH was only4% when compared to oxytocics. Result: This risk difference was well within therange of expected results for all uterotonic agents and does not warrant brandingmisoprostol as an inferior drug. Conclusion: Conventional uterotonic drugs shouldnot be used to set the lowest-accepted level of effectiveness in settings wherethey are entirely unsuitable. Continuing to weigh the benefits of one effectivedrug against another only delays the distribution of misoprostol in countries whereit is the only feasible choice and must be measured against no treatment at all.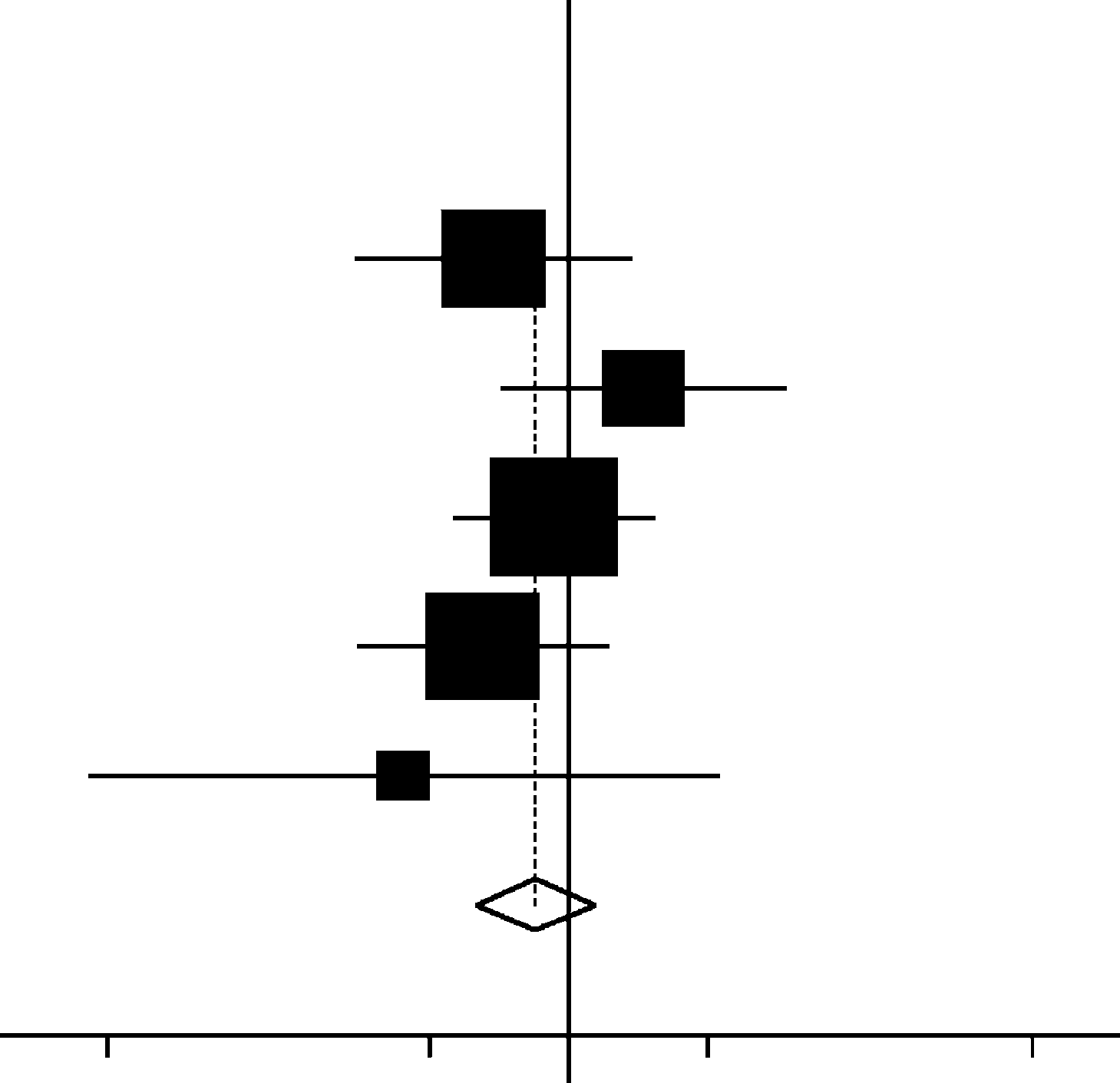 a One included study only reported outcome measurements for 500 mL.
a One included study only reported outcome measurements for 500 mL.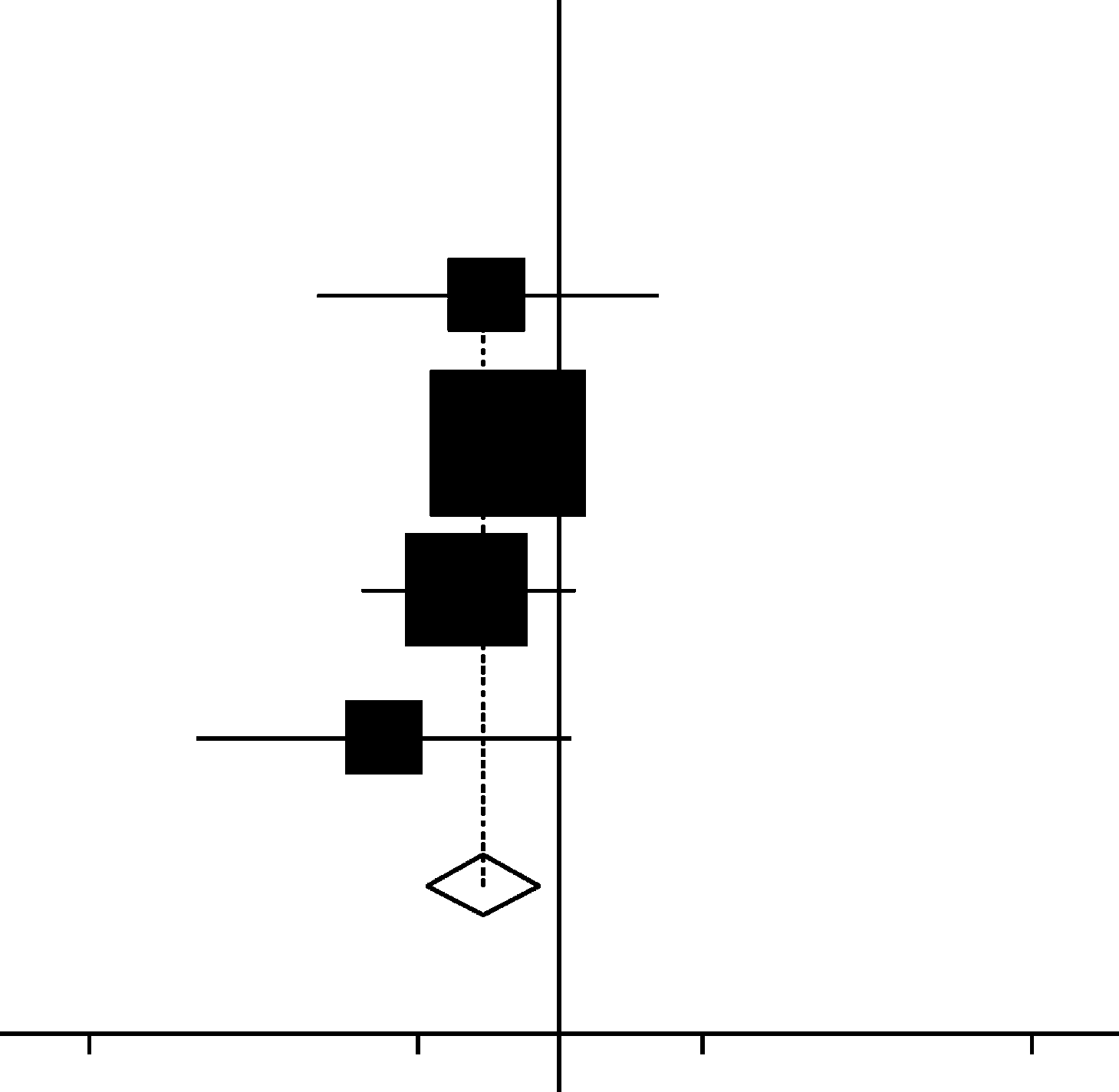 Misoprostol in preventing postpartum hemorrhage: A meta-analysis
All studies evaluating misoprostol vs. placebo with outcome of additional uterotonic agents. Mantel—
Haenszel fixed-effects model. Heterogeneity chi-squared = 1.62 (df = 3), p = 0.654. I-squared (variation in RRattributable to heterogeneity) = 0.0%. Test of RR = 1: z = 2.71, p = 0.007.
Misoprostol in preventing postpartum hemorrhage: A meta-analysis
All studies evaluating misoprostol vs. placebo with outcome of additional uterotonic agents. Mantel—
Haenszel fixed-effects model. Heterogeneity chi-squared = 1.62 (df = 3), p = 0.654. I-squared (variation in RRattributable to heterogeneity) = 0.0%. Test of RR = 1: z = 2.71, p = 0.007.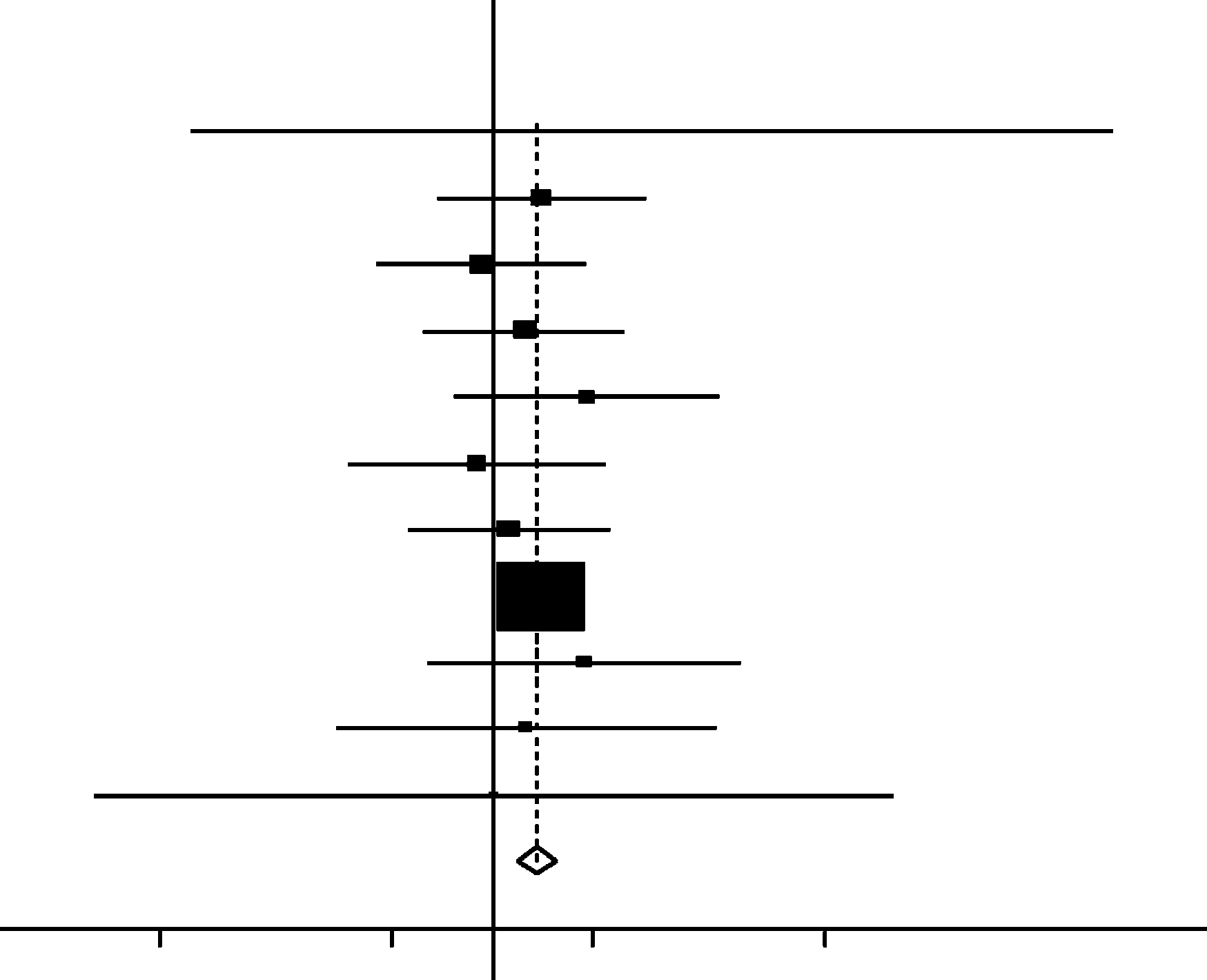
 All studies evaluating misoprostol vs. oxytocics with outcome blood loss N1000 mL. Mantel—Haenszel fixed-
effects model. Heterogeneity chi-squared = 3.64 (df = 10), p = 0.962. I-squared (variation in RR attributable toheterogeneity) = 0.0%. Test of RR = 1: z = 4.41, p = 0.000.
All studies evaluating misoprostol vs. oxytocics with outcome blood loss N1000 mL. Mantel—Haenszel fixed-
effects model. Heterogeneity chi-squared = 3.64 (df = 10), p = 0.962. I-squared (variation in RR attributable toheterogeneity) = 0.0%. Test of RR = 1: z = 4.41, p = 0.000.