La spécificité du tadalafil est liée à sa longue demi-vie, permettant une action qui excède largement celle des autres inhibiteurs de PDE5. L’absorption digestive est complète, avec un pic plasmatique atteint en 2 heures environ. Le métabolisme est réalisé via CYP3A4, produisant des métabolites inactifs éliminés principalement dans les fèces. La sélectivité enzymatique est élevée, réduisant les effets indésirables extra-caverneux. Les réactions indésirables fréquentes incluent céphalées, bouffées vasomotrices et troubles digestifs légers. L’activité pharmacologique est stable, indépendamment de l’ingestion d’aliments. Dans les comparaisons de longue durée, acheter cialis pas cher est mentionné en relation avec les études portant sur la persistance d’efficacité et la constance de la cinétique plasmatique.
Doi:10.1016/j.annemergmed.2005.08.007
A Clinical Prediction Rule for Early Discharge
From the University of British Columbia (Christenson, Innes, McKnight, Thompson, Wong,
Yu, Boychuk, Grafstein, Rosenberg, Gin, Anis, Singer); St. Paul’s Hospital (Christenson,Innes, Thompson, Boychuk, Grafstein, Rosenberg); Vancouver Hospital (McKnight, Gin); and
the Center for Health Evaluation and Outcome Sciences (Christenson, Innes, Grafstein,
Wong, Yu, Anis, Singer) Vancouver, British Columbia, Canada.
Study objective: Current risk stratification tools do not identify very-low-risk patients who can be safelydischarged without prolonged emergency department (ED) observation, expensive rule-out protocols, orprovocative testing. We seek to develop a clinical prediction rule applicable within 2 hours of ED arrivalthat would miss fewer than 2% of acute coronary syndrome patients and allow discharge within 2 to3 hours for at least 30% of patients without acute coronary syndrome.
Methods: This prospective, cohort study enrolled consenting eligible subjects at least 25 years old at asingle site. At 30 days, investigators assigned a diagnosis of acute coronary syndrome or no acutecoronary syndrome according to predefined explicit definitions. A recursive partitioning model includedrisk factors, pain characteristics, physical and ECG findings, and cardiac marker results.
Results: Of 769 patients studied, 77 (10.0%) had acute myocardial infarction and 88 (11.4%) definiteunstable angina. We derived a clinical prediction rule that was 98.8% sensitive and 32.5% specific. Patients have very low risk of acute coronary syndrome if they have a normal initial ECG, no previousischemic chest pain, and age younger than 40 years. In addition, patients at least 40 years old andwith a normal ECG result, no previous ischemic chest pain, and low-risk pain characteristics have verylow risk if they have an initial creatine kinase-MB (CK-MB) less than 3.0 mg/L or an initial CK-MB greaterthan or equal to 3.0 mg/L but no ECG or serum-marker increase at 2 hours.
Conclusion: The Vancouver Chest Pain Rule for early discharge defines a group of patients who can besafely discharged after a brief evaluation in the ED. Prospective validation is needed. [Ann Emerg Med. 2006;47:1-10.]
0196-0644/$-see front matterCopyright ª 2006 by the American College of Emergency Physicians. doi:10.1016/j.annemergmed.2005.08.007
of 241 (4.6%) missed cases of acute myocardial infarction
and 10 of 157 (6.4%) cases of missed unstable angin
Approximately 15% to 25% of patients who present to
Chest pain units reduce the rate of missed myocardial infarction
emergency departments (EDs) with undifferentiated chest pain
but do so in part by including very-low-risk patients in
prove to have acute coronary syndrome within 30 days. US data
extensive rule-out myocardial infarction proto
suggest that 2.1% of patients with acute myocardial infarction
Many investigators have developed chest pain risk
and 2.3% of patients with unstable angina are initially
stratification tools. Goldman et aldeveloped a clinical/ECG
misdiagnosed,whereas a recent Canadian study identified 11
algorithm that identified patients with less than 7% risk of acute
Clinical Prediction Rule for Early Discharge of Chest Pain Patients
without acute coronary syndrome were discharged less than
What is already known on this topicAlthough several algorithms and computer programs
have been developed for emergency department (ED)
Clinical prediction rules are decisionmaking tools for
patients with potential acute coronary syndrome, none
clinicians that contain elements of the medical history, physical
has achieved sufficient accuracy to allow safe and rapid
examination, and simple diagnostic tests.An objective clinical
discharge of ED chest pain patients.
prediction rule to identify very-low-risk patients with chestpain who can be safely discharged without prolonged ED
observation, expensive rule-out protocols, or provocative
This study developed a clinical decision rule to identify
testing is needed. Such a rule would help reduce emergency
low-risk ED chest pain patients who can be safely
crowding, minimize patient inconvenience, and improve
discharged within 2 hours of presentation. This study did
cost-effectiveness of acute coronary syndrome diagnostic testing.
not prospectively evaluate this rule.
Our specific objective was to develop a clinical prediction
Not surprisingly, this study found that patients younger
rule that would improve on current practice by identifying
than 40 years and with normal initial ECG results and no
patients with chest pain who are safe for discharge after 2 hours
previous ischemic chest pain were at very low risk of acute
of ED evaluation. The rule will miss fewer than 2% of acute
coronary syndrome. Additionally, patients older than
coronary syndrome patients and allow discharge within 2 to
40 years had low-risk if they had a normal ECG result, no
3 hours of at least 30% of patients without acute coronary
previous ischemic chest pain, low risk chest pain
characteristics, and an initial creatine kinase-MB(CK-MB) less than 3.0 ug/L or an initial CK-MB greater
than 3.0 ug/L but without an increase or ECG changes
Using established methodology for clinical prediction
rules,this prospective cohort study was conducted in 2
This derivation study should not change clinical practice
separate periods between June 29, 2000, and January 24, 2003,
because it has not yet been validated. It does, however,
when research assistants were funded.
provide support for the general belief that young patientswith a normal ECG result and no cardiac risk factors are
at very low risk of an adverse cardiovascular event.
Patients presenting to St. Paul’s Hospital, an urban tertiary
care ED, with a primary complaint of anterior or lateral chestpain were eligible for the study. Research assistants obtained
myocardial infarction. Limkakeng et subsequently found
informed consent and enrolled eligible patients between 7 AM
that 4.9% of patients who had low-risk Goldman criteria
and 10 PM 7 days per week. Patients were excluded if they were
and a negative initial troponin I assay result experienced death,
younger than 25 years, had a clear traumatic or radiologically
acute myocardial infarction, or revascularization within 30 days.
evident cause, were enrolled in the study in the previous 30
Pozen et aldeveloped a 7-item predictive equation that
days, had a terminal noncardiac illness, had severe
reduced coronary care unit admissions but not inappropriate
communication problems, were without a fixed address in the
discharges. Selker et modified this to create the acute
province of British Columbia, or were without available
cardiac ischemia time-insensitive predictive instrument
telephone contact. The Providence Health Care Research Ethics
(ACI-TIPI), which defined low risk as less than 10% chance
of acute coronary syndrome. The Erlanger protocis anintense 2-hour assessment that includes serial ECGs and
creatine kinase-MB (CK-MB) and troponin measurements,
This report conforms to the published standard reporting
but it does not define a subset of patients who can forgo
guidelines for studies evaluating risk stratification of ED
nuclear stress testing. The American Heart Association/Agency
patients with potential acute coronary syndalthough
for Health Care Policy and Research guidelines suggest early
they were developed before this publication. A total of 123
discharge only for patients with ‘‘evidence’’ of an alternate
potential predictor variables were screened (). During
diagnosis.Unfortunately, few patients clearly fall into this
the first 2 hours of the index visit, research assistants
category. Our own study of patients with chest pain at 2
documented vital signs every 30 minutes, initiated ST-segment
Vancouver hospitals identified that 5.4% of patients with
monitoring, and ensured that serial ECGs (0, 1, and 2 hours)
acute coronary syndrome were discharged from the ED without
were performed. Cardiac markers at 0 and 2 hours were
a diagnosis or planned investigations and only 30% of those
evaluated on several platforms: creatine phosphokinase (Access,
Clinical Prediction Rule for Early Discharge of Chest Pain Patients
Pain and Associated Symptom Characteristics
Parent or sibling with heart attack \65 years
2-h ST segment monitoring (any ST elevation or ST depression)*
Difference in CPK (2 h–0 h) (Standard)*
Difference in Tn I or T (2 h–0 h) (Standard)*
Difference in CK-MB (2 h–0 hour) (Biosite)*
Difference in myoglobin (2 h–0 h) (Biosite)*
Pain diagnosed in past as either AMI or angina
Previous angiogram yes and previous lesion O50%*
Did pain improve within 5 minutes of nitroglycerin?*
Did pain improve within 5 minutes of oxygen?
Did pain improve within 5 minutes of liquid antacid?
During 2 hours, did pain relieve and not return?*
Right arm systolic pressure, left arm systolic pressure
Systolic pressure \90 mm Hg in 2 hoursBradycardia \50 beats/min in 2 hours*
Figure 1. List of all predictors collected for possible inclusion in
the prediction rule. Those meeting criteria for inclusion in the
model are identified with an asterisk.
AMI, Acute myocardial infarction; Hx, history; MI, myocardial
infarction; PCI, percutaneous coronary intervention; CABG, coronary
artery bypass graft; CVA, cerebrovascular accident; TIA, transientischemic attack; ASA, acetyl salicylic acid; ACE, angiotensin-converting enzyme.
Clinical Prediction Rule for Early Discharge of Chest Pain Patients
Table 1. Baseline characteristics and outcomes of patient
Table 2. Univariate predictive statistics for predictors used in
Mean pulse rate on arrival (beats/minGSD)
Mean respiratory rate on arrival (breaths/minGSD)
% With pain radiating to left arm, jaw, or neck
% With pain increasing with a deep breath
% With any increase in CK-MB during 2 hours
No acute coronary syndrome or adverse event
Mortality with definite unstable angina (%)
Mortality with possible unstable angina (%)
Mortality with no acute coronary syndrome
Mortality with no acute coronary syndrome
Beckman Coulter, Mississauga, Ontario, Canada), troponin I
(Access and Biosite Triage, San Diego, CA), troponin T
(Roche Elecsys, Hoffman LaRoche, LaValle, Quebec, Canada),
*Predictors with an odds ratio O1 indicate that the predictor is associated with an
myoglobin (Biosite Triage), and CK-MB (Biosite Triage).
increased risk of acute coronary syndrome. y‘‘ECG normal’’ is defined as no ST-segment deviation and no T-wave inversion
Serum markers ordered by research protocol but not for
regardless of conditions such as left ventricular hypertrophy or left bundle-branch
clinical purposes were unavailable to clinicians. They acquired
block. T-wave flattening was not defined as abnormal.
chest pain characteristics, patient risk factors, and medicalhistory independently of clinicians and recorded physicalfindings determined by emergency physicians, provisional
intervention, chest compressions, percutaneous intervention,
emergency diagnosis, admission and discharge times,
and coronary artery bypass grafting.
consultations, cardiac medications administered, other cardiac
Interobserver reliability was estimated by having a second
investigations, hospital discharge diagnoses, and predefined
emergency physician blindly evaluate 95 patients.
At 30 days, research staff telephoned patients to review
Adverse events included death, tachycardia requiring
current medications, physician visits, and hospital visits. Reports
intervention, bradycardia requiring intervention, assisted
of all diagnostic tests performed during the 30 days in any
ventilations, proven pulmonary thromboembolism, proven
setting were obtained, and relevant physicians were contacted
aortic aneurysm or dissection, new congestive heart failure
for confirmation of any new diagnoses. In cases in which patient
requiring intravenous therapy, hypotension requiring
contact was lost, other city hospital records were reviewed to
Clinical Prediction Rule for Early Discharge of Chest Pain Patients
identify hospital visits, procedures, and new diagnoses, and the
pre- or postmorbid investigation. The diagnosis of definite
study list was cross-referenced against the British Columbia
unstable angina required rest pain greater than or equal to 20
minutes and at least 1 of the following related to the presentingsymptoms: (1) troponin increase 0.1 to 0.99 mg/L but no other
acute myocardial infarction criteria, (2) dynamic ECG changes
Investigators used predefined explicit criteria to assign a
consistent with ischemia in 2 contiguous leads (dynamic ST
30-day outcome diagnosis of acute myocardial infarction, definite
depression O0.5 mm or dynamic deep T-wave inversion) but no
unstable angina, possible unstable angina, or no acute coronary
persistent ST elevation, (3) a coronary angiogram with greater
syndrome. The primary outcome was definite acute coronary
than 70% lesion plus hospital admission for acute coronary
syndrome (acute myocardial infarction or definite unstable
syndrome, or (4) a positive stress test result (radionuclide scan,
angina). The diagnosis of acute myocardial infarction required
echo, or ECG stress test) plus admission for acute coronary
any one of the following: (1) a CK-MB increase definite for
acute myocardial infarction based on the specific hospital
If a diagnosis could not be assigned or if an investigator
criteria or troponin I level greater than or equal to1.0 mg/L;
assigned a diagnosis of ‘‘no acute coronary syndrome’’ despite
(2) a troponin I increase (O0.1 mg/L but \1.0 mg/L) with
objective criteria (eg, positive troponin assay result), or if an
dynamic ECG changes consistent with ischemia, a coronary
investigator assigned a diagnosis of ‘‘definite unstable angina’’
angiogram with greater than 70% lesion, a positive stress test
based only on a positive troponin assay result, 2 cardiologist
result (radionuclide scan, echocardiogram, or ECG), or urgent
coinvestigators independently reviewed all clinical data and
revascularization; (3) ECG evolution consistent with acute
assigned an adjudicated outcome diagnosis. If necessary, final
myocardial infarction; (4) fibrinolytic therapy or primary
diagnosis was based on agreement of any 2 adjudicators and the
angioplasty and a clinical diagnosis of acute myocardial
principal investigator. If all 3 disagreed, the final outcome was
infarction; or (5) death with no other definite cause found in
Clinical Prediction Rule for Early Discharge of Chest Pain Patients
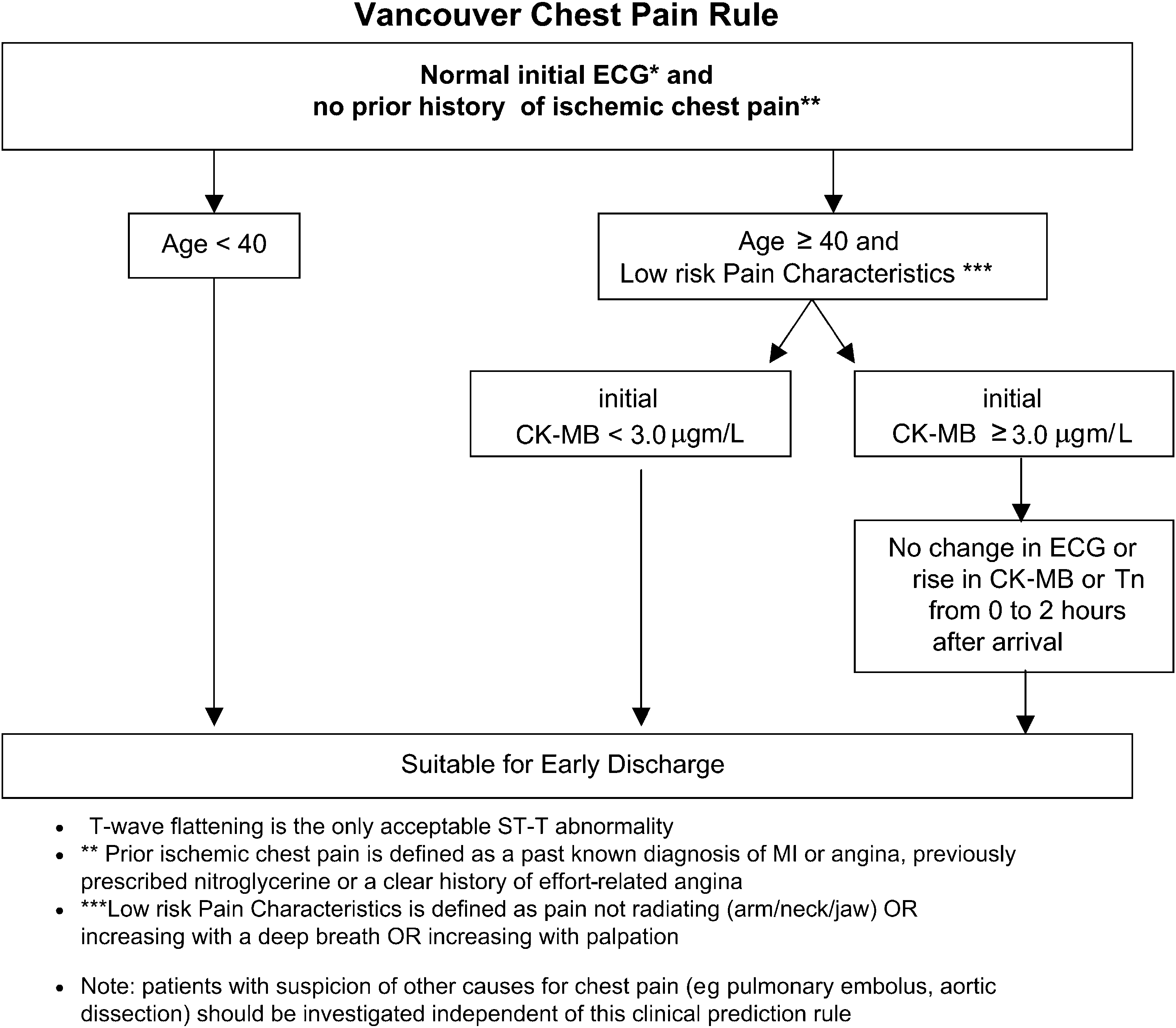
Figure 3. Chest pain early discharge rule.
Investigators reviewed all ECGs in a structured format to
predictors were chosen initially by the algorithm and then
identify T-wave flattening, T-inversion in 2 contiguous leads,
rounded to convenient values by the investigators, and the
ST depression (R0.05 mV) in 2 contiguous leads, ST-elevation
patients were reclassified based on rounded values. Predictor
(R0.1 mV in limb leads or R0.2 mV in precordial leads), and
variables were allowed in the model if they were univariately
the presence of left bundle-branch block, paced rhythm, or left
associated with the primary outcome (P\.2). In addition,
ventricular hypertrophy. In addition, investigators blinded to
variables subjected to interpretation (medical history and
final outcome reviewed all ECGs for each patient and recorded
physical examination findings) were included if they were
their impression of the likelihood of ischemia. Evaluation of all
reliable (lower bound of confidence [95%] was at least 0.4 for
available ECGs was used for outcome determination.
the reliability measure; prevalence and bias adjusted k
Evaluation of ECGs up to 2 hours was used as predictors
coefficient for dichotomous variables and intraclass correlation
coefficient for continuous variables).
Investigators reviewed each derived rule for clinical relevance.
Nodes with small numbers of patients were reaggregated and
Data were collected on specific study data forms and entered
recursive partitioning was reinstituted to simplify the branch
into an Oracle database (Oracle Corporation, Redwood City,
points. This modification, although not previously described,
CA, USA). Proportions, medians, means, and SDs were
makes clinical sense and reduces the chance of selecting a
calculated and multiple clinical prediction rules were derived
nonoptimal splitting variable when partitioning groups with
using the S-Plus (Insightful Corp., Seattle, WA) ‘‘rpart’’
smaller sample sizes. The simplest, most specific prediction
recursive partitioning module. The algorithm was run using all
rule that met the goal of sensitivity greater than 98% was
of the default options except that a 10:1 loss was specified for
missed acute coronary syndrome patients versus missed non-
We do not report confidence intervals (CI) around the
acute coronary syndrome patients. This higher penalty on
sensitivity and specificity values, because these values arise as a
missed acute coronary syndrome patients encouraged the
consequence of the rule development process, not as an
algorithm to choose splits that maximized sensitivity and so
evaluation of a fixed rule. Specifically, the sampling variability
reduce the complexity of the model. Cut points for continuous
in the estimated sensitivity cannot be assessed because different
Clinical Prediction Rule for Early Discharge of Chest Pain Patients
samples lead to different rules (all of which are forced to satisfy
the ‘‘at least 98% sensitive’’ criterion). Meaningful CIs will be
The sample size of 800 patients was chosen so that equal
numbers would be used in rule development and in subsequent
rule validation. In the validation phase, the aim is to confirm
that the sensitivity of the rule exceeds current practice (ie, to
obtain a lower bound on the 95% CI for sensitivity of acute
coronary syndrome detection that is no less than 0.95).
Assuming that the true sensitivity is of the rule is 0.98, roughly
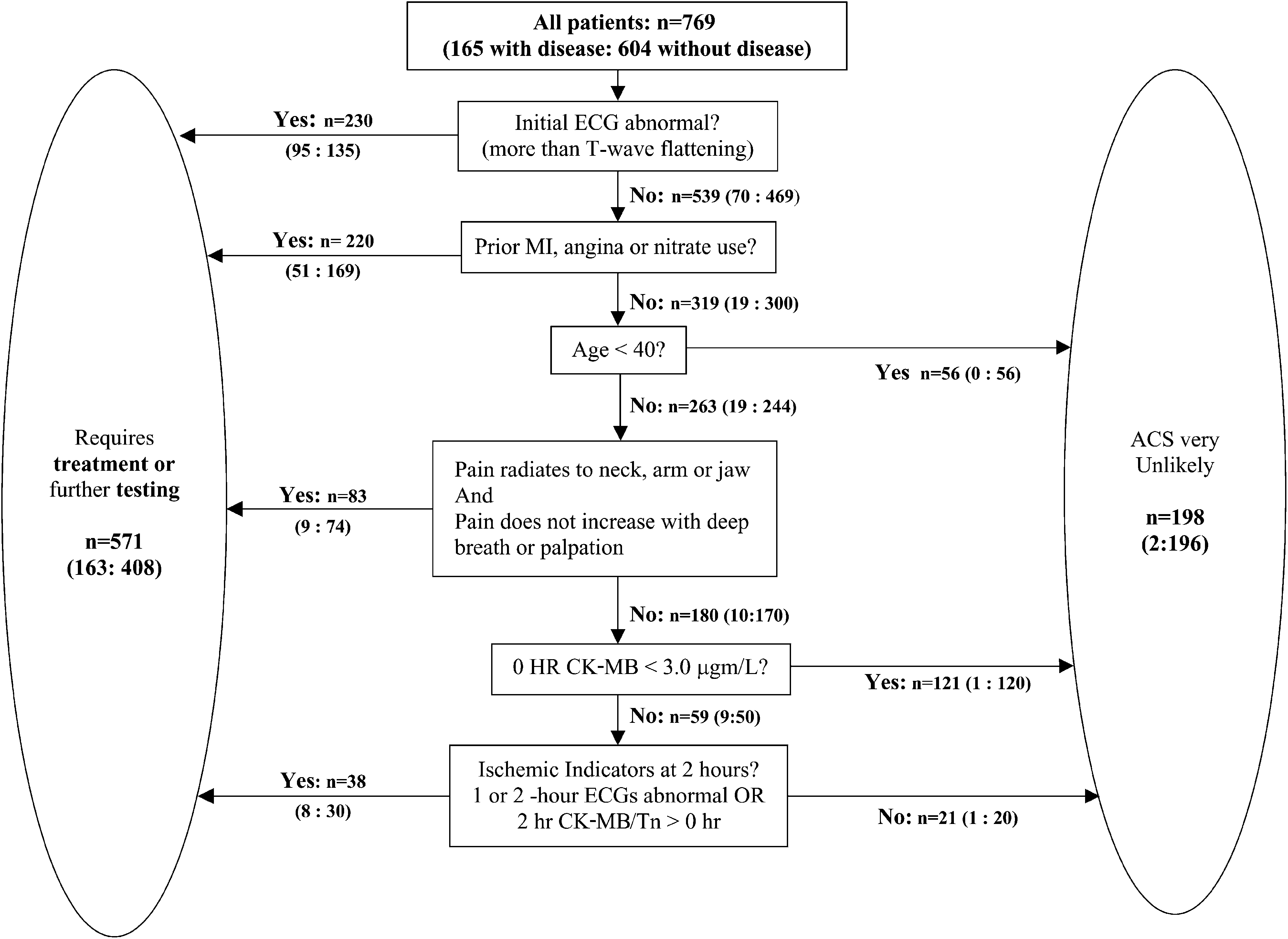
*Sensitivity 98.8%; specificity 32.5%; positive predictive value 28.5%; negative
187 positive cases (800 patients in total) are needed to achieve
this lower bound with 90% probability.
allows the early discharge process to be divided into
We enrolled 819 patients and subsequently excluded
The 2 missed patients were subsequently diagnosed with
50 patients from analysis, 31 who met exclusion criteria and 19
unstable angina. A 66-year-old woman was diagnosed 8 days
who were lost to follow-up. Of the 19 lost to follow-up, 14 were
later by outpatient nuclide stress testing, with no subsequent
known to be alive at subsequent hospital visits, and the other 5
admission or adverse event. The other was a 52-year-old patient
did not appear in the provincial death registry.
with a clear history of new and accelerating angina before rest
summarizes baseline characteristics and outcomes for the 769
pain who was treated medically for a single critical lesion not
patients analyzed showing 30-day diagnosis was acute
amenable to intervention. During validation, we will clarify the
myocardial infarction in 77 (10.0%) and definite unstable
definition of past angina to include a recent history of typical
angina in 88 (11.4%). Documented adverse events related or
angina of effort whether diagnosed or not.
unrelated to acute coronary syndrome included tachycardia(35), bradycardia (14), assisted ventilations (4), proven
pulmonary thromboembolism (5), proven thoracic aortic
Although we used accepted and validated methodology,
aneurysm or dissection (0), new congestive heart failure
the Vancouver Chest Pain Prediction Rule was developed in
requiring intravenous therapy (12), hypotension requiring
1 cohort of patients in a single center. We are currently
intervention (9), and chest compressions (2). Eighty-three
beginning validation of the rule, and it will subsequently
patients had percutaneous intervention and 31 had coronary
require evaluation of implementation in multiple centers. Our
artery bypass grafting within 30 days.
criterion standard for definite acute coronary syndrome was
Of the 123 possible predictor variables screened, 48 were
not based on mandated investigations but on a careful
retained for entry into the recursive partitioning algorithm.
evaluation of all tests and visits during 30 days. It is possible that
lists the variables selected for the rule by diagnostic
we missed some patients with silent events. The cohort was
groups with respective univariate statistics and P values. These
collected during day and evening hours and will require
variables include a normal ECG result (which could include
validation in patients presenting at all hours of the day. The rule
T-wave flattening but no ST deviation or T-wave inversion), age,
is modestly complex and may be difficult to remember, which
previous ischemic pain, 3 pain descriptors, 1 physical finding,
could limit its use by clinicians. However, the rule is largely
and both CK-MB and troponin results. Reliability measures
intuitive, and simple memory aids (eg, pocket cards or PDA
(95% CI) for clinical subjective variables were pain radiates to
algorithms) will enhance implementation once the rule is
neck, 0.68 (95% CI 0.54 to 0.83); pain radiates to jaw, 0.81
validated. It is important to note that although our focus was on
(95% CI 0.69 to 0.93); pain radiates to left arm, 0.79 (95% CI
identifying patients with very low risk of acute coronary
0.67 to 0.91); and chest tenderness reproduces pain, 0.63 (95%
syndrome, no patients were missed with pulmonary embolism
or aortic dissection. Suspicion of other life-threatening
outlines the classification tree, and is a
conditions requires appropriate, independent investigations.
simplified clinical algorithm of the chest pain prediction rule.
In retrospect, this rule development should have included
In this development cohort, the rule is 98.8% sensitive,
patients 24 hours per day. Ideally, the study would be
identifying all but 2 patients with unstable angina, and would
strengthened by mandating initial and 30-day imaging
have allowed the appropriate discharge of 32.5% of patients
studies to improve the criterion standard of acute coronary
without acute coronary syndrome using data collected within 2
syndrome. The cost implications of the Vancouver Chest
hours of arrival (Of those identified for discharge,
89.4% would be determined with information available atpresentation, most without any laboratory testing, and the
remainder would be determined safe for discharge based on
Patients who present to the ED with chest pain fall into
repeat ECG, CK-MB, and troponin at 2 hours. This potentially
3 categories: those with objective ischemia who need admission
Clinical Prediction Rule for Early Discharge of Chest Pain Patients
and treatment, those with a clear noncardiac cause, and those
Recent American College of Cardiology/American Heart
who require a diagnostic process to rule out acute coronary
Associationguidelines recommend that all patients with a
syndrome and other life-threatening conditions. The Vancouver
compatible history have serial marker testing until 9 hours after
Chest Pain Rule identifies 32.5% of patients who do not have
symptom onset, followed by provocative testing. Applying this
acute coronary syndrome using information available in the
guideline in the ED, where most patients have ill-defined
first 2 hours of the ED visit. These very-low-risk patients are
chest discomfort, could greatly increase diagnostic and ED bed
identified with minimal error, in fact including only 1.2% of
utilization without a corresponding improvement in patient
those who do have unstable angina or acute myocardial
outcomes. The ED/AHCPR guidelines and the Toronto Heart
infarction. This information can be integrated into the decision
Centre ACS Guidelinesrecommend excluding patients with
framework of the emergency physician who continually
discomfort because of other causes from the diagnostic pathway,
evaluates patients for safe and appropriate disposition.
but neither suggests a process for identifying these patients.
This prediction rule is different from previous risk
The Vancouver Chest Pain Rule is unique in its ability to
stratification tools. In 1988, Goldman et aldeveloped a
identify very-low-risk patients who are suitable for early
clinical/ECG algorithm that identified patients with less than
discharge. It is also unique in that it identifies patients in a
7% risk of acute myocardial infarction. This was not designed
clinically logical stepwise process with a minimum of
to detect patients with unstable angina and it did not improve
investigations. First, age, initial history, and ECG findings
disposition decisions relative to experienced clinician judgment
identified 56 of 198 patients who ultimately meet rule criteria.
alone. Limkakeng et allater reported that 4.9% of patients
A further 121 patients were identified based on initial CK-MB
with low-risk Goldman criteria and a negative initial troponin
and low-risk pain characteristics. The last 21 patients were
I level experienced death, acute myocardial infarction, and
identified by the absence of changes in the ECG or serum
revascularization within 30 days. Lee et aland Goldman et al
markers during 2 hours. If disposition according to the rule was
subsequently developed a strategy to identify patients
implemented in this stepwise manner, ED lengths of stay and
unlikely to have acute myocardial infarction and criteria to
investigational costs could be reduced substantially in many
identify patients who need coronary care unit admission. These
criteria required 12 to 24 hours of observation and did not
Some would argue that the age criteria might result in
facilitate early ED disposition decPozen et al
missing younger patients with myocardial infarction, but age is
developed and tested a predictive equation using 7 clinical
in fact a powerful predictor, and the low-risk group younger
and ECG variables. After application of this instrument,
than 40 years is also defined by a near-normal ECG and the
inappropriate coronary care unit admissions fell from 24% to
absence of past myocardial infarction or angina. Marsan et al
17%, but the 3% inappropriate discharge rate was unchanged.
recently studied 1032 patients younger than 40 years and
Selker et almodified the Pozen et alequation and linked
presenting with chest pain and found that those with no
it to ECG findings, creating an electronic tool called the
cardiac history and either no cardiac risk factors or a normal
ACI-TIPI. This tool increased the rate of appropriate
ECG result had less than 0.5% 30-day risk of acute coronary
discharges by unsupervised residents but did not change
the performance of attending physicians. Of note,
We found that CK-MB at a low threshold was consistently a
ACI-TIPI defines low risk as less than 10% chance of acute
better discriminator than any level of troponin, surprising
myocardial infarction or unstable angina, and few clinicians will
because many studies suggest troponin is the superior marker.
Our findings are not unique, and at least 1 other investigator
In 1992, Baxtand Baxt and Skora‘‘trained’’ neural
has reported that CK-MB was more predictive of acute coronary
networks to recognize acute myocardial infarction and, in 1993,
syndrome than troponin early in the patient’s presentati
Jonsbu et developed a sensitive computer-derived
Laboratory technicians used the Triage (Biosite) point-of-care
algorithm. Doyle et studied 9 algorithms but found none
device, and we attribute the greater discriminatory power of
that improved clinical decisionmaking. The recently described
CK-MB over troponin to its better analytic performance within
Thrombolysis in Myocardial Infarction (TIMI) Risk scoreis
the normal range. The reported 99th percentile for troponin
an excellent stratification tool but was derived from studies of
on the Triage point-of-care device is actually the detection
patients with objective evidence of acute coronary syndrome
limit (0.19 mg/L), whereas the 95th percentile for CK-MB
and has not been validated in undifferentiated ED patients with
(usual cutoff) is well above the detection limit (0.75 mg/L).
chest discomfort. The Erlanger protocolis an intense 2-hour
de Winter et determined that an increase in CK-MBmass
assessment that includes serial ECGs, 2 CK-MB and troponin
greater than 2 mg/L represents the critical difference between
measurements, clinical judgment, and nuclear stress testing.
2 results for the detection of myocardial damage. We
It is the most detailed published protocol designed to facilitate
hypothesize that it is the absence of a critical increase over
early discharge but requires nuclear imaging to increase
baseline value (median 1.5 mg/L) that underlies the
sensitivity from 80% to 99%. None of the above stratification
discriminatory power of a CK-MB level less than 3 mg/L. In
tools help clinicians identify patients who are safe to discharge
comparison, present troponin methods do not permit the
detection of a change within the normal range.
Clinical Prediction Rule for Early Discharge of Chest Pain Patients
An early discharge strategy such as the one developed here
6. Goldman L, Cook E, Brand D. A computer protocol to predict
defines patients safe for early discharge and reduces the number
myocardial infarction in emergency department patients with chestpain. N Engl J Med. 1988;318:797-803.
who require more definitive testing but also defines the
7. Limkakeng A Jr, Gibler WB, Pollack C, et al. Combination of
companion group of patients who are not clearly ‘‘safe’’ and
Goldman risk and initial cardiac troponin I for emergency
require further investigations. To maximize diagnostic
department chest pain patient risk stratification. Acad Emerg Med.
efficiency, a more prolonged ‘‘chest pain unit’’ rule-out strategy
should be applied to patients without objective ischemia who do
8. Pozen MW, D’Agostino RB, Selker HP, et al. A predictive instrument to
improve coronary-care-unit admission practices in acute
ischemic heart disease: a prospective multicenter clinical trial. N Engl J
In summary, the Vancouver Chest Pain Rule defines a group
of chest pain patients who can be safely discharged from the
9. Pozen MW, D’Agostino RB, Mitchell JB, et al. The usefulness of a
ED in the first few hours after arrival. If validated in an
predictive instrument to reduce inappropriate admissions to the
independent cohort, it will improve the process of diagnostic
coronary care unit. Ann Intern Med. 1980;92:238-242.
10. Selker HP, Beshansky JR, Griffith JL, et al. Use of the acute cardiac
decisionmaking in patients presenting with chest pain.
ischemia time-insensitive predictive instrument (ACI-TIPI) to assistwith triage of patients with chest pain or other symptoms
The authors are grateful for the support and data supplied by the
suggestive of acute cardiac ischemia: a multicenter, controlled
physicians and nurses at St. Paul’s Hospital, Vancouver, Canada,
clinical trial. Ann Intern Med. 1998;129:845-855.
and for the dedication of Patti Lawson, BA, and Courtney Barker.
11. Selker H, D’Agostino R, Laks M. A predictive instrument for acute
ischemic heart disease to improve coronary care unit admissionpractices: a potential on-line tool in a computerized
Supervising editor: Judd E. Hollander, MD
electrocardiograph. J Electrocardiol. 1988;(21 suppl):S11-S17.
12. Selker H, Griffith J, Patil S, et al. A comparison of performance of
Author contributions: DM, HR, EY, EG, FR, AA, and JS helped
mathematical predictive methods for medical diagnosis: identifying
design the study, analyzed the data, and reviewed the
acute cardiac ischemia among emergency department patients.
manuscript. BB helped design the study, collected data, and
reviewed the manuscript. JMC, GI, and CRT conceived and
13. Fesmire FM, Hughes AD, Fody EP, et al. The Erlanger chest pain
helped design the study, collected data, and wrote the
evaluation protocol: a one-year experience with serial 12-lead ECG
manuscript. JMC takes responsibility for the paper as a whole.
monitoring, two-hour delta serum marker measurements, andselective nuclear stress testing to identify and exclude acute
Funding and support: Canadian Institutes of Health research
coronary syndromes. Ann Emerg Med. 2002;40:584-594.
grant MOP 53102 and Heart and Stroke Foundation of British
14. Braunwald E, Antman E, Beasley J, et al. ACC/AHA: a guideline
Columbia and Yukon Grant. Materials for analysis of some
update for the management of patients with unstable angina and
laboratory testing were donated by Biosite.
non-ST-elevation myocardial infarction: a report of the AmericanCollege of Cardiology/American Heart Association task force on
Publication dates: Received for publication March 17, 2005.
practice guidelines (committee on the management of patients
Revision received June 13, 2005. Accepted for publication July
13, 2005. Available online October 19, 2005.
15. Laupacis A, Sekar N, Stiell IG. Clinical prediction rules: a review and
Reprints not available from the authors.
suggested modifications of methodological standards. JAMA.
Address for correspondence: Jim Christenson, MD, Department
16. Wasson J, Sox H, Neff R, et al. Clinical prediction rules: application
of Emergency Medicine, St. Paul’s Hospital, 1081 Burrard
and methodologic standards. N Engl J Med. 1985;313:793-799.
Street, Vancouver, British Columbia V6Z 1Y6, Canada; 604-
17. Stiell IG, Wells GA. Methodologic standards for the development of
clinical decision rules in emergency medicine. Ann Emerg Med.
18. Hollander JE, Blomkalns AL, Brogan GX, et al. Standardized
reporting guidelines for studies evaluating risk stratification of ED
1. Pope J, Aufderheide T, Ruthazer R, et al. Missed diagnoses of acute
patients with potential acute coronary syndromes. Acad Emerg
cardiac ischemia in the emergency department. N Engl J Med.
19. Lee TH, Juarez G, Cook EF, et al. Ruling out acute myocardial
2. Christenson J, Innes G, McKnight D, et al. Safety and efficiency of
infarction: a prospective multicenter validation of a 12-hour
emergency department assessment of chest discomfort. CMAJ.
strategy for patients at low risk. N Engl J Med. 1991;324:
3. Anderson HJ. Hospitals battle heart attacks with new chest pain
20. Goldman L, Cook EF, Johnson PA, et al. Prediction of the need for
intensive care in patients who come to the emergency departments
4. Zalenski RJ, Rydman RJ, Ting S, et al. A national survey of
with acute chest pain. N Engl J Med. 1996;334:1498-1504.
emergency department chest pain centers in the United States.
21. Reilly B, Durairaj L, Husain S, et al. Performance and potential
impact of a chest pain decision prediction rule in a large public
5. Graff L, Joseph T, Andelman R, et al. American College of
hospital. Am J Med. 1999;106:285-291.
Emergency Physicians information paper: chest pain units in
22. Davis MA, Keerbs A, Hoffman JR, et al. Admission decisions
emergency departments: a report from the Short-Term
in emergency department chest pain patients at low risk for
Observation Services Section. Am J Cardiol. 1995;76:
myocardial infarction: patient versus physician preferences.
Clinical Prediction Rule for Early Discharge of Chest Pain Patients
23. Baxt WG. Analysis of the clinical variables driving decision in
28. Fesmire F, Hughes A, Fody E, et al. The Erlanger chest pain
an artificial neural network trained to identify the presence of
evaluation protocol: a one-year experience with serial 12-lead ECG
myocardial infarction. Ann Emerg Med. 1992;21:1439-1444.
monitoring, two-hour delta serum marker measurements, and
24. Baxt WG, Skora J. Prospective validation of artificial neural network
selective nuclear stress testing to identify and exclude acute
trained to identify acute myocardial infarction. Lancet. 1996;347:
coronary syndromes. Ann Emerg Med. 2002;40:584-594.
29. Fitchett D, Goodman S, Langer A. New advances in the management
25. Jonsbu J, Aase O, Rollag A, et al. Prospective evaluation of
of acute coronary syndromes. CMAJ. 2001;164:1309-1316.
an EDB-based diagnostic program to be used in patients
30. Marsan R, Shaver K, Sease K, et al. Validation of a clinical decision
admitted to hospital with acute chest pain. Eur Heart J. 1993;
rule for young adult chest pain patients. Acad Emerg Med. 2004;
26. Doyle Y, Conroy R, Mulcahy R. Can we improve on the diagnostic
31. Svensson L, Isaksson L, Axelsson C, et al. Predictors of myocardial
accuracy of chest pain in accident and emergency departments?
damage prior to hospital admission among patients with acute
chest pain or other symptoms raising a suspicion of acute coronary
27. Holper E, Antman E, McCabe C, et al. A simple, readily available
syndrome. Coron Artery Dis. 2003;14:225-231.
method for risk stratification of patients with unstable angina and
32. de Winter RJ, Koster RW, van Straalen JP, et al. Critical difference
non-ST elevation myocardial infarction. Am J Cardiol. 2001;87:
between serial measurements of CK-MB mass to detect myocardial
Stiftung zum Schutze unserer Fledermäuse in der Schweiz Foundation for Bat Conservation in Switzerland Fondation pour la protection des chauves-souris en Suisse Fondazione per la protezione dei pipistrelli della Svizzera Fundaziun per la protecziun da noss mez mieurs e mez utschels en Svizra Liste der empfohlenen und für Fledermäuse verträglichen Holzschutzmittel Empfohlen werden al
Saw Palmetto Extracts for Treatment of Benign Prostatic Hyperplasia A Systematic Review Timothy J. Wilt, MD, MPH; Areef Ishani, MD; Gerold Stark, MD; Roderick MacDonald, MS; Joseph Objective.— To conduct a systematic review and, where possible, quantitative meta-analysis of the existing evidence regarding the therapeutic efficacy and safety of the saw palmetto plant extra
 Clinical Prediction Rule for Early Discharge of Chest Pain Patients
identify hospital visits, procedures, and new diagnoses, and the
pre- or postmorbid investigation. The diagnosis of definite
study list was cross-referenced against the British Columbia
unstable angina required rest pain greater than or equal to 20
minutes and at least 1 of the following related to the presentingsymptoms: (1) troponin increase 0.1 to 0.99 mg/L but no other
acute myocardial infarction criteria, (2) dynamic ECG changes
Investigators used predefined explicit criteria to assign a
consistent with ischemia in 2 contiguous leads (dynamic ST
30-day outcome diagnosis of acute myocardial infarction, definite
depression O0.5 mm or dynamic deep T-wave inversion) but no
unstable angina, possible unstable angina, or no acute coronary
persistent ST elevation, (3) a coronary angiogram with greater
syndrome. The primary outcome was definite acute coronary
than 70% lesion plus hospital admission for acute coronary
syndrome (acute myocardial infarction or definite unstable
syndrome, or (4) a positive stress test result (radionuclide scan,
angina). The diagnosis of acute myocardial infarction required
echo, or ECG stress test) plus admission for acute coronary
any one of the following: (1) a CK-MB increase definite for
acute myocardial infarction based on the specific hospital
If a diagnosis could not be assigned or if an investigator
criteria or troponin I level greater than or equal to1.0 mg/L;
assigned a diagnosis of ‘‘no acute coronary syndrome’’ despite
(2) a troponin I increase (O0.1 mg/L but \1.0 mg/L) with
objective criteria (eg, positive troponin assay result), or if an
dynamic ECG changes consistent with ischemia, a coronary
investigator assigned a diagnosis of ‘‘definite unstable angina’’
angiogram with greater than 70% lesion, a positive stress test
based only on a positive troponin assay result, 2 cardiologist
result (radionuclide scan, echocardiogram, or ECG), or urgent
coinvestigators independently reviewed all clinical data and
revascularization; (3) ECG evolution consistent with acute
assigned an adjudicated outcome diagnosis. If necessary, final
myocardial infarction; (4) fibrinolytic therapy or primary
diagnosis was based on agreement of any 2 adjudicators and the
angioplasty and a clinical diagnosis of acute myocardial
principal investigator. If all 3 disagreed, the final outcome was
infarction; or (5) death with no other definite cause found in
Clinical Prediction Rule for Early Discharge of Chest Pain Patients
identify hospital visits, procedures, and new diagnoses, and the
pre- or postmorbid investigation. The diagnosis of definite
study list was cross-referenced against the British Columbia
unstable angina required rest pain greater than or equal to 20
minutes and at least 1 of the following related to the presentingsymptoms: (1) troponin increase 0.1 to 0.99 mg/L but no other
acute myocardial infarction criteria, (2) dynamic ECG changes
Investigators used predefined explicit criteria to assign a
consistent with ischemia in 2 contiguous leads (dynamic ST
30-day outcome diagnosis of acute myocardial infarction, definite
depression O0.5 mm or dynamic deep T-wave inversion) but no
unstable angina, possible unstable angina, or no acute coronary
persistent ST elevation, (3) a coronary angiogram with greater
syndrome. The primary outcome was definite acute coronary
than 70% lesion plus hospital admission for acute coronary
syndrome (acute myocardial infarction or definite unstable
syndrome, or (4) a positive stress test result (radionuclide scan,
angina). The diagnosis of acute myocardial infarction required
echo, or ECG stress test) plus admission for acute coronary
any one of the following: (1) a CK-MB increase definite for
acute myocardial infarction based on the specific hospital
If a diagnosis could not be assigned or if an investigator
criteria or troponin I level greater than or equal to1.0 mg/L;
assigned a diagnosis of ‘‘no acute coronary syndrome’’ despite
(2) a troponin I increase (O0.1 mg/L but \1.0 mg/L) with
objective criteria (eg, positive troponin assay result), or if an
dynamic ECG changes consistent with ischemia, a coronary
investigator assigned a diagnosis of ‘‘definite unstable angina’’
angiogram with greater than 70% lesion, a positive stress test
based only on a positive troponin assay result, 2 cardiologist
result (radionuclide scan, echocardiogram, or ECG), or urgent
coinvestigators independently reviewed all clinical data and
revascularization; (3) ECG evolution consistent with acute
assigned an adjudicated outcome diagnosis. If necessary, final
myocardial infarction; (4) fibrinolytic therapy or primary
diagnosis was based on agreement of any 2 adjudicators and the
angioplasty and a clinical diagnosis of acute myocardial
principal investigator. If all 3 disagreed, the final outcome was
infarction; or (5) death with no other definite cause found in
 Clinical Prediction Rule for Early Discharge of Chest Pain Patients
Figure 3. Chest pain early discharge rule.
Clinical Prediction Rule for Early Discharge of Chest Pain Patients
Figure 3. Chest pain early discharge rule.