Microsoft word - new patient clinical information form, final, 14mar03.doc
William R. Klemme, M.D.
Diplomat, American Board of Orthopaedic SurgeryPractice Limited to Spine Surgery Adult and Pediatric Spine Surgery Degenerative and Deformity ConditionsNEW PATIENT CLINICAL INFORMATION FORM
Is your problem related to: Job injury
Briefly describe your main problem/complaint. Also, describe the injury that caused these symptoms, if applicable. How long have you had this problem? FOR PHYSICIAN USE ONLY - HISTORY OF PRESENT ILLNESS (These are preliminary notes; refer to dictation for more details)
Outpatient Center, Suite A, 1125 Sir Francis Drake Blvd., Kentfield, California 94904
Office: 415-485-3500 • Fax: 415-456-0456 • www.williamklemme.md
Using the symbols below, please draw in the location of your symptoms on the diagrams. X = Pain ○ = Numbness / = Aching • = Pins & Needles
If you have NECK PAIN, what percentage is: % Neck and % Arm (Total 100%) If you have ARM PAIN, is this: Right arm Left arm Both arms If you have BACK PAIN, what percentage is:
If you have LEG PAIN, is this: Right leg Left leg Both legs
IF APPLICABLE, mark an X on the line to indicate your usual degree of pain (0 meaning NO PAIN and 10 meaning WORST PAIN) NECK PAIN: 0_____1_____2_____3_____4_____5_____6_____7_____8_____9_____10
ARM PAIN: 0_____1_____2_____3_____4_____5_____6_____7_____8_____9_____10
BACK PAIN: 0_____1_____2_____3_____4_____5_____6_____7_____8_____9_____10
LEG PAIN: 0_____1_____2_____3_____4_____5_____6_____7_____8_____9_____10
What position/activity makes the pain worse/better? WORSE
How long can you STAND with no or minimal pain: ______minutes. WALKING DISTANCE with no or minimal pain: 0-50ft _____ 50-200 ft _____ 200-500 ft ____ 500+ ft ____ 1/2 mile+ _____ Do you need SUPPORT to help you walk? _____Yes _____No If yes, what kind of support? Do you wear a back or neck BRACE? _____Yes _____No If yes, what kind of brace?
List below the PREVIOUS PHYSICIANS (MD, DO, Chiropractor) you have seen for your main complaint/problem.
Indicate which DIAGNOSTIC TESTS you have had in evaluation of your main complaint/problem (please include dates).
Please check which TREATMENTS you have had for your main problem/complaint and indicate whether they were helpful.
√ Helpful? Treatment √ Helpful? Treatment √ Helpful?
PAST MEDICAL HISTORY: Please check below if you have had any of the following:
List any SURGERIES you have had.
DRUG ALLERGIES:
List ALL CURRENT MEDICATIONS as follows:
(milligrams, grams) (how many times a day)
Have you taken any of the following drugs previously?
√ Helpful? Medication √ Helpful? Medication √ Helpful?
SOCIAL HISTORY & HABITS:
Occupation: ____________________ Marital Status: Single Married Divorced Number of Children: _____ Highest Education Level: High School Equivalency High School Graduate WORK STATUS:
Full Duty Limited Duty Off Duty per physician Unemployed Retired If you are NOT working FULL DUTY, how long have you been off work? ________________ Have you had a work capacity assessment? ____Yes ____ No Are you disabled through Social Security? ____ Yes ____ No TOBACCO USE:
Do you currently use Tobacco products? ____Yes ____ No Started Age/Year: __________ If yes, indicate the quantity per day: Cigarettes _____________ Cigars______________ Chewing Tobacco (snuff) ____________ Have you stopped using Tobacco products? ____ Yes ____ No If so, When? ___________ ALCOHOL USE:
Do you currently consume alcoholic beverages? ____Yes ____ No If yes, indicate the quantity per day: Beer _________________ Wine ________________ Distilled spirits ________________ Have you ever been treated for drug or alcohol addiction? ____ Yes ____ No REVIEW OF SYSTEMS: Check if you have experienced any of the following: CONSTITUTIONAL EYES, EAR, NOSE √ RESPIRATORY GASTROINTESTINAL GENITO-URINARY CENTRAL NERVOUS CARDIOVASCULAR MUSCULOSKELETAL
FAMILY HISTORY: Describe current health, age, cause of death, illness, diabetes, cancer, hypertension, etc. FEMALE PATIENTS:
Date of last MENSTRAL PERIOD: ________________________ MALE PATIENTS:
Date of last PROSTATIC EXAM: _________________________
Rectal test: _____ Yes _____ No Results: _________________________________________ PSA (prostate blood test) _____ Yes _____ No Results: ______________________________
The preceding patient information packet has been reviewed and discussed with my patient.
Safety Precautions of 3V Lithium Coin Cells Lithium Manganese Dioxide Coin Cell contains flammable materials, such as organics solvent. Improper battery handling may cause leakage, heating, explosion or ignition of the battery, which may lead to injury or product failure. Please read and observe the following precautions in designing and mounting thoroughly. Precaution in Designing ● Do
Page - 1 - of 8 SDV8000 Laboratory trials 2009 AN INVESTIGATION OF THE ANTIMICROBIAL EFFICIENCY OF SAGE SYSTEMS STEAM AND VACUUM CLEANING SYSTEM “SAGE STEAM” Information and statistics reproduced with permission of copyright holder Page - 2 - of 8 SDV8000 Laboratory trials 2009 1.0 Introduction Sage Sanitizing Systems Ltd are in the business of providing technological s
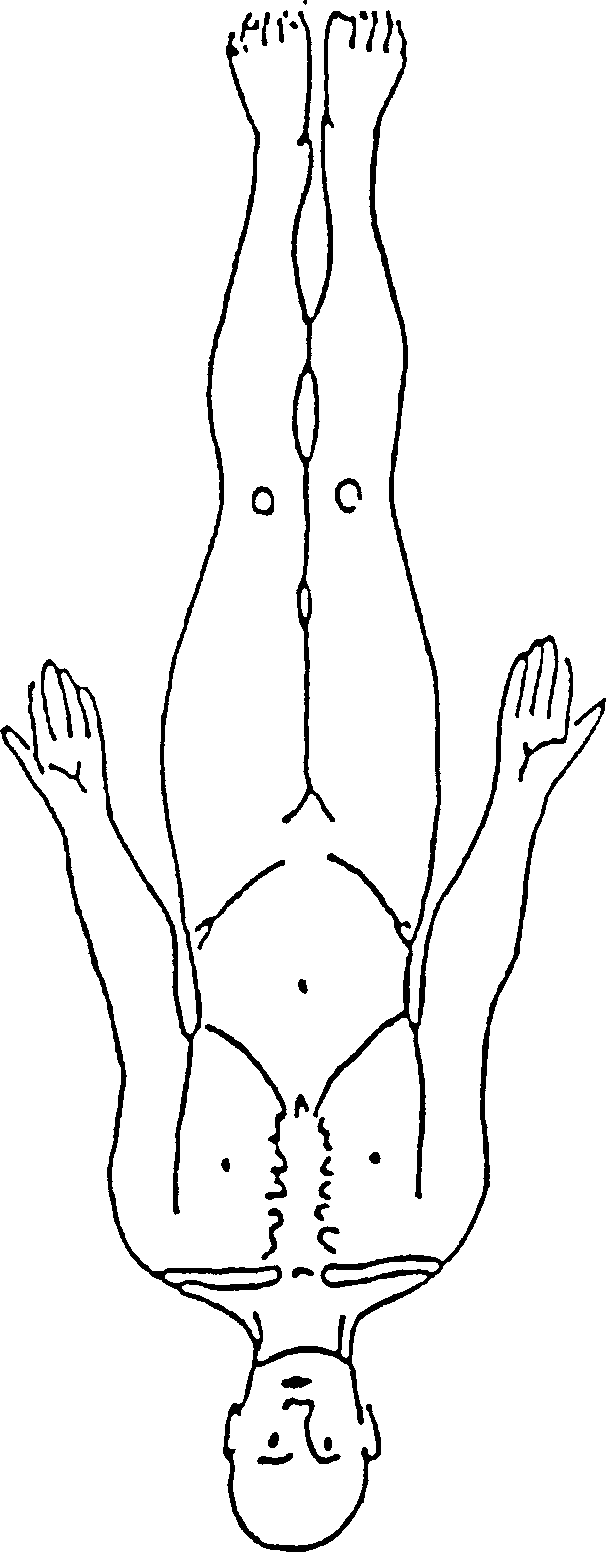
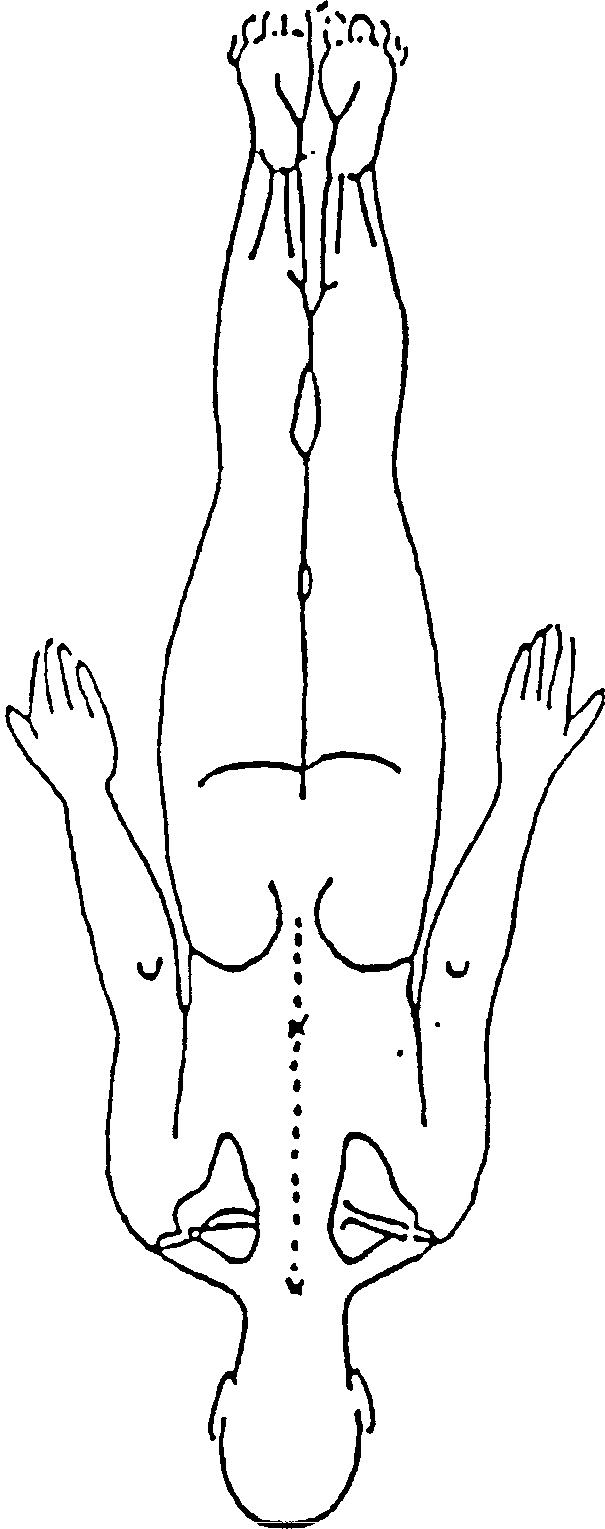 Using the symbols below, please draw in the location of your symptoms on the diagrams.
Using the symbols below, please draw in the location of your symptoms on the diagrams.