La spécificité du tadalafil est liée à sa longue demi-vie, permettant une action qui excède largement celle des autres inhibiteurs de PDE5. L’absorption digestive est complète, avec un pic plasmatique atteint en 2 heures environ. Le métabolisme est réalisé via CYP3A4, produisant des métabolites inactifs éliminés principalement dans les fèces. La sélectivité enzymatique est élevée, réduisant les effets indésirables extra-caverneux. Les réactions indésirables fréquentes incluent céphalées, bouffées vasomotrices et troubles digestifs légers. L’activité pharmacologique est stable, indépendamment de l’ingestion d’aliments. Dans les comparaisons de longue durée, acheter cialis pas cher est mentionné en relation avec les études portant sur la persistance d’efficacité et la constance de la cinétique plasmatique.
ACTA oTorhinolAryngologiCA iTAliCA:EPUB February 09, 2012
Case report Pseudomonas and Aspergillus interaction in
malignant external otitis: risk of treatment failureInterazione tra Pseudomonas ed Aspergillus nell’otite esterna maligna: rischio di fallimento terapeuticoR. Bovo, A. BenAtti, A. CioRBA1, M. LiBAnoRe2, M. BoRReLLi3, A. MARtinient – ear Surgery Unit, Az. ospedaliera Padova, italy; 1 Audiology Unit, Ferrara University, italy; 2 infectious Disease
Unit, Ferrara University, italy; 3 neuroradiology Unit, Ferrara University, italy
malignant external otitis (mEo) is a rare infection of the temporal bone primarily affecting elderly patients and diabetics or immunocom-promised individuals, which may have dismal prognosis if treatment is not prompt and adequate. Almost 95% of mEo cases reported in the literature are attributed to Pseudomonas aeruginosa, and this pathogen is isolated from aural drainage in > 90% of cases. however, in recent years fungal and polymicrobial temporal bone infections have been reported with increasing frequency. The aim of this paper is to discuss a possible pitfall in mEo treatment using an unusual clinical case. in this patient, bacteriological data positive for Pseudomonas delayed correct diagnosis of Aspergillus infection, which was obtained after surgical debridement and biopsy of the infra-temporal space.
KEy wordS: Necrotizing otitis externa • Diagnosis and prognosis • AspergillusL’otite esterna maligna (MEO) è una rara infezione dell’osso temporale che colpisce soprattutto pazienti anziani e diabetici o individui immunocompromessi, che può avere prognosi infausta se il trattamento non è rapido e adeguato. Quasi il 95% dei casi di MEO riportati in letteratura sono attribuiti a Pseudomonas aeruginosa e questo patogeno è isolato dal materiale di drenaggio auricolare in più del 90% dei casi. Tuttavia negli ultimi anni infezioni polimicrobiche e micotiche dell’osso temporale sono sempre più frequenti. Scopo di questo lavoro è discutere del rischio di fallimento terapeutico nell’otite esterna maligna attraverso l’illustrazione di un caso clinico in cui il tampone auricolare positivo per Pseudomonas ha ritardato la diagnosi della infezione da Aspergillus, ottenuta dopo un debridement chirurgico dello spazio infra-temporale.
PArolE ChiAvE: Otite esterna maligna • Diagnosi e prognosi • Aspergillus
Acta Otorhinolaryngol Ital:EPUB February 09, 2012
Introduction
date. histologically, granulation tissue is characterized by non-specific inflammation with inflammatory cell infiltra-
malignant external otitis (mEo) is a rare infection of the tion and hyperplasia of squamous epithelium.
temporal bone primarily affecting elderly patients and The progression of the disease has been divided into 3
diabetics or immunocompromised individuals, which may have dismal prognosis if treatment is not prompt and clinical stages as shown in Table i 4. in the third stage, the adequate. Pseudomonas aeruginosa is responsible for al-
infection reaches the intracranial structures, neck spaces
most all cases, although a few cases may be due to other and large blood vessels. This stage is always associated microorganisms (Aspergillus species, Staphylococcus au-
with poor prognosis. The most frequent causes of death
reus, Klebsiella oxytoca, and others) 1-3.
are meningitis, large vessel septic thrombophlebitis or
The disease manifests as a painful inflammation of the rupture, septicaemia, pneumonia caused by inhalation for external ear canal, associated with purulent otorrhea and vagal paralysis and cerebrovascular accident 5 6. granulation polyps. otalgia is the presenting symptom in The aim of this paper is to discuss a possible pitfall in 75% of cases; it is intense, particularly during the night, mEo treatment using an unusual clinical case. in this pa-and associated with a severe temporal or occipital head-
tient, the bacteriological data positive for Pseudomonas
ache. The purulent otorrhea appears with a frequency delayed correct diagnosis of Aspergillus infection, which ranging from 50 to 80% and varies from a moist and mod-
was obtained after surgical debridement and biopsy of the
est secretion to a greenish malodorous and abundant exu-
Table I. Clinical-radiological stages of malignant external otitis. Stage I: infection of the external auditory canal and adjacent soft tissues
with severe pain, with or without facial nerve paralysis. Stage II: extension of infection with osteitis of skull base and temporal
bone, or multiple cranial nerve neuropathies. Stage III: intracranial extension with meningitis, epidural empyema,
Clinical case Between 1992 and 2009, 8 patients affected by mEo have been treated at our department. The causative pathogen was Pseudomonas aeruginosa in all cases except in the one presented, where Pseudomonas was associated with Aspergillus fumigatus. in 2006, a 69-year-old insulin-dependent individual with diabetes presented to our clinic complaining of otalgia and otorrhoea lasting for 2 months, despite repeated treatment Fig. 1. Axial CT showing soft tissue involvement of the right external and with systemic antibiotic and local antiseptic irrigation. on the middle ear with bone erosion. Enlargement of the right foramen lacerum examination, the right ear canal was full of purulent se-
and condyloid canal, as well the facial nerve canal, can be observed.
cretion, oedematous and occupied by extensive granula-tion tissue, the tympanic membrane was hyperaemic and thickened. Ear discharge was cultured for bacteria and mycosis with isolation of P. aeruginosa. The patient had no fever and blood cultures were not performed. Blood ex-amination demonstrated ESr = 142 mm; CrP = 116 mg/l; wBC = 12.45 × 109/l. mri demonstrated a diffuse inflam-mation of temporal bone cavities, while CT excluded bone erosions. he was treated with aural toilet on a regular ba-sis, ciprofloxacin 750 mg (Bid) and control of diabetes, but two weeks later, when still on treatment, he developed right facial paresis. The ear swab was repeated and was positive for P. aeruginosa. A meatoplasty with mastoido-tympanoplasty to remove the infected and necrotic tissue was carried out. moreover, EPUB
dosage of 2 gr (Tid) and continued for 2 weeks. Although a control ear swab was negative for bacterial infection, the previous treatment with ciprofloxacin was continued. Four months later the patient was still on treatment, when he manifested a paralyses of glossopharyngeal and vagus Fig. 2. T1 weighted with contrast magnetic resonance, axial section. Patho-
nerves. mri demonstrated pathologic tissue occupying logical tissue on T1 weighted images with contrast enhancement involves
the right cranial base, widening the jugular foramen, and the neotympanic cavity, the lateral parapharyngeal space, the right posterior the retropharyngeal space reaching the omolateral clivus, foramen lacerum, as well as the condyloid canal. It also extends posteriorly while CT scans disclosed bone erosion extending beyond involving the right cerebellum (arrow). the previous surgical mastoidectomy (Figs. 1, 2). The patient underwent skull base surgical debridement and a ESr = 15 mm; CrP = 16 mg/l; wBC = 6.25 × 109/l. Fur-specimen of infratemporal tissue demonstrated non-spe-
thermore, glossopharyngeal and vagus nerve function be-
cific inflammation, while bacterial examination and cul-
came normal. The treatment was maintained for 3 months:
ture grew A. fumigatus. voriconazole was administered at at this time, complete normalization by mri was dem-a dosage of 400 mg i.v. twice for the first day, followed by onstrated, together with resolution of clinical signs and 200 mg i.v. (Bid). After one month of antifungal therapy, normalization of biochemical indexes of inflammation. there was significant clinical improvement in general con-
Follow-up was carried out with regular mri and blood ex-
ditions, control of diabetes and reduction of otalgia and amination. After 4 years of follow-up, there are no signs of headache. inflammation indices were reduced as follows: disease although the facial paresis persists. Pseudomonas and Aspergillus interaction in malignant external otitis
Discussion
vasive aspergillosis during therapy 11. Unfortunately, false positivity may be related to antibiotic treatment 12, while
malignant external otitis is an insidious disease with false negativity may be observed in immunocompromised
frequently delayed diagnosis, so that patients are often patients. in the past, mri has been used in association
treated for a trivial external otitis. Almost 95% of mEo with other imaging modes for diagnosis and follow-up of
cases reported in the literature are attributed to P. aeru-
mEo (i.e. Tc-99mdP bone scanning, ga-76 citrate scan-
ginosa, and this pathogen is isolated from aural drainage ning and gallium-67 SPECT). however, mri has many
in > 90% of cases 1 3. however, in recent years fungal and advantages over other modalities and can be used as the
polymicrobial temporal bone infections have been re-
sole imaging modality 13. in our case, a temporal bone CT
ported with increasing frequency 1-3. in fact, P. aeruginosa carried out after the clinical worsening of disease demon-
is frequently a saprophyte in the external auditory mea-
strated bone erosion that was not present initially. moreo-
tus and sometimes other associated bacteria or fungi can ver, mri was repeated several times during treatment and
have an important or predominant role in the aetiology of follow-up with good monitoring of disease evolution.
mEo, particularly in immunocompromised patients, such when mEo is suspected, patients have been generally
as in AidS, where Pseudomonas is not the predominant started on empirical antipseudomonal therapy due to the
high incidence of this causative pathogen. Ciprofloxacin
Although fungal infections are generally more invasive is still the treatment of choice, although increasing re-
than bacterial disease, all the other clinical and radiologi-
sistance is observed among Pseudomonas strains. in our
cal features, including survival, are similar 2 3 8. Thus, even district, 9.5% of Pseudomonas strains isolated from ear
the isolation of Pseudomonas from aural discharge may swabs are resistant to ciprofloxacin. Thus, we still use this
be not sufficient or specific enough to distinguish between antibiotic empirically in external otitis when Pseudomonas
the two forms. As emphasized by leonetti and marzo 9 pa-
aetiology is suspected and microbiological data are lack-
tients are either referred with previous cultures and biopsy ing. nevertheless, the incidence of antibiotic resistance
findings or are extremely tender on external auditory mea-
should be regularly monitored in each hospital district.
tus manipulation; general anaesthesia is required to obtain Antibiotic therapy is associated with regular external ear
an adequate biopsy. For these reasons, it is tempting to canal cleaning in micro-otoscopy and medicated washes.
rely either on previous findings or on bacteriologic data to There is no role for topical antibiotics, even quinolones,
direct therapy. As a consequence, Pseudomonas isolation in the treatment of mEo. instillation of antipseudomonal
may delay correct diagnosis of fungal infection 10.
topical agents only increases the difficulty of isolating the
gillus is also frequently isolated pathogenic organism from the ear canal.
from external auditory canal smears and diagnosis of fun-
on the other hand, topical antibiotics are generally rec-
gal mEo should be based on histopathologic confirma-
ommended for bacterial external otitis, but it should be
tion on deep tissue biopsy or isolation from blood cul-
considered that the incidence of mycotic forms has sig-
tures or fistula exudates 10. no diagnostic conclusions can nificantly risen since the end of 1990’s, when the use of
be drawn from single positive cultures from the external quinolone ear drops became common clinical practice 14.
auditory canal or from middle ears with chronic perfora-
if a fungus is the causative organism, prolonged treatment
(> 12 weeks) with amphotericin B is indicated. A liposomal
Aspergillus identified in our patient was isolated on deep
amphotericin B preparation is recommended to keep to a
tissue specimens obtained at surgery: we assume they minimum the incidence of nephrotoxicity in diabetic pa-
were neither contaminated or secondary to prior antibi-
tients. more recently, voriconazole has demonstrated high
otic therapy. This peculiar case of mEo underlays the efficacy in mEo caused by Aspergillus species 15. hyper-
importance of performing repeated biopsies and culture baric oxygen has been used on occasion with mixed results,
to identify microorganisms, which can be different or as-
and may be considered as adjuvant treatment for refractory
sociated with the most common causative (i.e. P. aerugi-
cases although its efficacy remains unproven 4 16. nosa). often, multiple histologic sections are necessary The decision between conservative antimicrobial therapy for identifying fungi or other particular organisms.
and surgical treatment can present a therapeutic challenge
Blood tests are generally non-specific except for a con-
in the management of these life-threatening infections, es-
stant elevation of inflammatory indices: an elevated ESr pecially in patients with existing immunodeficiency and and CrP were present in 100% of patients and often illness 17. Although bone sequestra and abscess are treated reached values > 100. Conversely, leukocytosis is rare. surgically, the need for more aggressive treatment is de-ESr and CrP are also indicators of disease activity and batable. Some authors suggest that prompt surgical debri-are useful for monitoring the course of therapy and ef-
dement consisting of radical mastoidectomy is indicated
fectiveness of antibiotic treatment. recently, two different in the majority of cases, particularly in fungal diseases, markers, galactomannan and β-glucan have demonstrated which are more invasive with respect to bacterial patho-their value in diagnosis and monitoring the course of in-
in the series reported by hamzani 2, extensive surgery was 8 Barrow hn, levenson mJ. Necrotizing “malignant ” ex-carried out in 78% of fungal mEo vs. 18% in bacterial
ternal otitis caused by Staphylococcus epidermidis. Arch
ones. however, other authors stress the fact that exten-
otolaryngol head neck Surg 1992;118:94-6.
sive surgery may be even counterproductive because of 9 leonetti JP, marzo SJ. Invasive fungal and bacterial infections the risk of exposing healthy bone to infection 3 21. Unfor-
of the temporal bone. laryngoscope. 2003;113:1503-7.
tunately, there are neither guidelines nor definite recom-
10 martínez-Berriotxoa A, montejo m, Aguirrebengoa K, et al.
mendations with regard to the surgical treatment of the
Otomastoiditis caused by Aspergillus in AIDS. Enferm in-
different forms of mEo 22. in our case, we carried out extensive infratemporal debrid-
11 mokaddas E, Burhamah mh, Ahmad S, et al. Invasive pul-monary aspergillosis due to Aspergillus terreus: value of
ment which permitted a correct causative diagnosis through
DNA, galactomannan and (1->3)-beta-D-glucan detection
histological and bacteriological examination of tissues.
in serum samples as an adjunct to diagnosis. J med micro-
nevertheless, it remains questionable whether a more lim-
ited deep tissues biopsy followed by antifungal treatment 12 Boonsarngsuk v, niyompattama A, Teosirimongkol C, et al.
would have been sufficient to resolve the disease. False-positive serum and bronchoalveolar lavage Aspergil-
in conclusion, all cases of otitis externa by Pseudomonas
lus galactomannan assays caused by different antibiotics.
in elderly diabetic or immunocompromised patients
should be initially treated as potential forms of mEo. The 13 ismail h, hellier wP, Batty v. Use of magnetic resonance course of mEo is initially subtle, and the disease may
imaging as the primary imaging modality in the diagnosis
have poor prognosis if not properly treated. nevertheless,
and follow-up of malignant external otitis. J laryngol otol
no diagnostic conclusions can be drawn from single posi-
tive cultures from the external auditory canal. in fact, col-
martin TJ, Kerschner JE, Flanary vA. Fungal causes of oti-tis externa and tympanostomy tube otorrhea. int J Pediatr
onization with Pseudomonas, both in chronic otitis media
and in superficial external otitis is probably common, and 15 Parize P, Chandesris mo, lanternier F, et al. Antifungal
thus mycosis should be suspected whenever clinical signs
therapy of Aspergillus invasive otitis externa: efficacy of
of infection do not improve despite adequate anti-Pseu-voriconazole and review. Antimicrob Agents Chemother
domonas treatment. 2 5 23. in these cases, deep tissue biopsy
or isolation from blood cultures is required for histopatho-
16 Phillips JS, Jones SEm. Hyperbaric oxygen as an adjuvant treatment for malignant otitis externa. Cochrane database
References
17 Chen d, lalwani AK, house Jw, et al. Aspergillus mas-
toiditis in acquired immunodeficiency syndrome. Am J otol
lignant external otitis: clinical, radiological, and anatomic
18 Amonoo-Kuofi K, Tostevin P, Knight Jr. Aspergillus mas-
correlations. lancet infect dis 2004;4:34-9.
toiditis in a patient with systemic lupus erythematosus: a
hamzany y, Soudry E, Preis m, et al. Fungal malignant ex-case report. Skull Base 2005;15:109-12. ternal otitis. J infect 2011;62:226-31.
19 Sreepada gS, Kwartler JA. Skull base osteomyelitis second-
Carfrae mJ, Kesser Bw. Malignant otitis externa. otolaryn-
ary to malignant otitis externa. Curr opin otolaryngol head
davis JC, gates gA, lerner C, et al. Adjuvant hyperbaric
20 Soudry E, Joshua BZ, Sulkes J, et al. Characteristics and oxygen in malignant external otitis. Arch otolaryngol head
prognosis of malignant external otitis with facial paralysis.
Arch otolaryngol head neck Surg 2007;133:1002-4.
Chen Cn, Chen yS, yeh Th, et al. Outcomes of malignant
21 Amorosa l, modugno gC, Pirodda A. Malignant external external otitis: survival vs. mortality. Acta otolaryngol
otitis: review and personal experience. Acta otolaryngol
Soudry E, hamzany y, Preis m, et al. Malignant external oti-
22 walsh TJ, Anaissie EJ, denning dw, et al. Treatment of as-tis: analysis of severe cases. otolaryngol head neck Surg
pergillosis: clinical practice guidelines of the Infectious Dis-eases Society of America. Clin infect dis 2008;46:327-60.
ress Bd, luntz m, Telischi FF, et al. Necrotizing external oti-
23 vourexakis Z, Kos mi, guyot JP. Atypical presentations of tis in patients with AIDS. laryngoscope 1997;107:456-60. malignant otitis externa. J laryngol otol 2010;124:1205-8.
received: April 27, 2011 - Accepted: november 12, 2011
Address for correspondence: roberto Bovo, md, UoC di orl-otochirurgia, Az. ospedaliera, via giustiniani 2, 35128 Padova, italy. E-mail: [email protected]
[email protected] | www.ashleyfure.net | (b. 1982, USA) Harvard University – Cambridge, Massachusetts PhD Candidate in Music Composition, Expected Completion May 2013 Cursus 2, October 2010 – June 2011 Cursus 1, September 2008 – April 2009 Harvard University – Cambridge, Massachusetts Master of Arts in Music Composition with Distinction, June 2006 Bachelor of Music in
Behandeling op basis van risiconiveau´s De zorgketen bestaat uit een aantal verschil ende fasen die elkaar opvolgen in het zorgproces. Na de diagnose volgt de aanvul ende analyse van persoonsgegevens en het opstel en van het individueel zorgplan en de behandeling plus onderhoud, waarna de fase van begeleiding start. De interventies voor de behandeling van obesitas verschil en qua intens
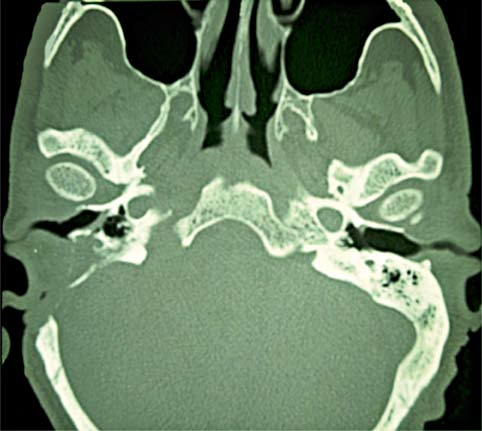
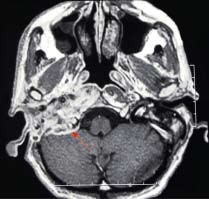 Table I. Clinical-radiological stages of malignant external otitis.
Table I. Clinical-radiological stages of malignant external otitis.