La spécificité du tadalafil est liée à sa longue demi-vie, permettant une action qui excède largement celle des autres inhibiteurs de PDE5. L’absorption digestive est complète, avec un pic plasmatique atteint en 2 heures environ. Le métabolisme est réalisé via CYP3A4, produisant des métabolites inactifs éliminés principalement dans les fèces. La sélectivité enzymatique est élevée, réduisant les effets indésirables extra-caverneux. Les réactions indésirables fréquentes incluent céphalées, bouffées vasomotrices et troubles digestifs légers. L’activité pharmacologique est stable, indépendamment de l’ingestion d’aliments. Dans les comparaisons de longue durée, acheter cialis pas cher est mentionné en relation avec les études portant sur la persistance d’efficacité et la constance de la cinétique plasmatique.
P-neb user guide 2008a
USER’S GUIDEP-NEB User’s Guide PercussiveNEB™ (P-NEB)
P-NEB is a high frequency intrapulmonary percussive nebulizer
intended for the clearance of endobronchial secretions. TABLE OF CONTENTS
Functional and Operational Characteristics . 2Figure 1 – Airway Clearing Technique . 2
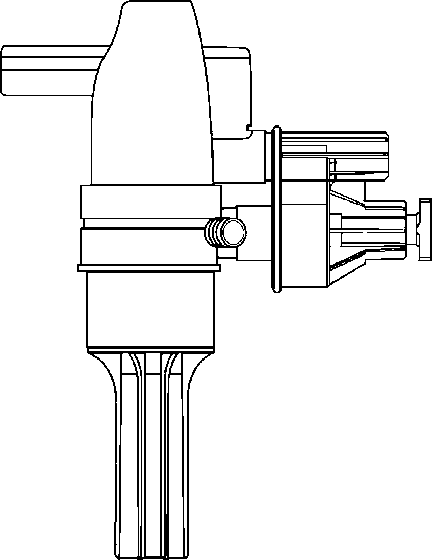
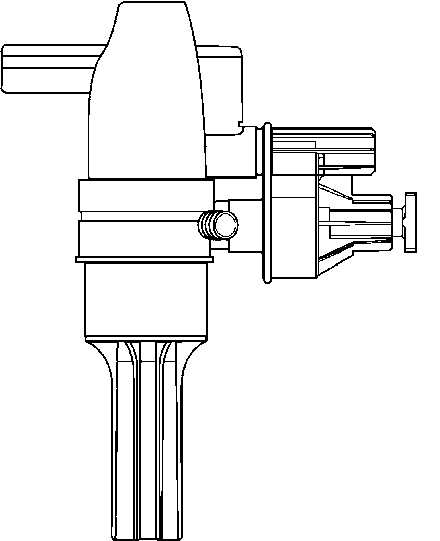
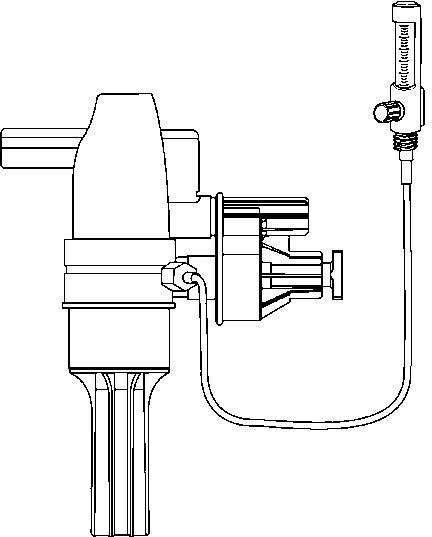
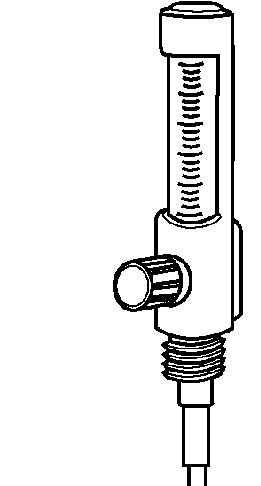
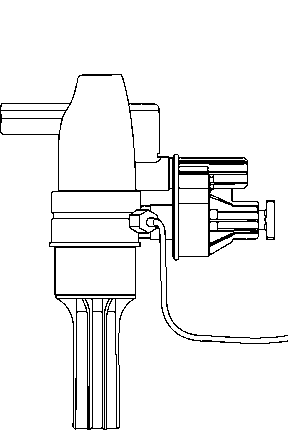
Clinical Considerations . 3Figure 2 - Connect P-NEB to a Flowmeter . 4Figure 3 - Component Description . 5
Protocol: Setup Instructions - PercussiveNEB. 6
VORTRAN Medical Technology 1, Inc. 21 Golden Land Court, Sacramento, CA 95834-2426 Tel: (800) 434-4034 P-NEB User’s Guide Functional and Operational Characteristics The PercussiveNEB is an intrapulmonary percussive treatment device that incorporates a nebulizer to deliver aerosolized medication and is designed to oscillate during exhalation and inhalation to help remove endobronchial se- cretions. During inhalation, the patient entrains high density aerosol from the nebulizer with high frequency intrapulmonary percussion for enhance aerosol deposition. The moisture and the medication in the aerosol help thin and mobilize secretions. During exhalation the pneumatic capacitor and pulmo- nary modulator cycle to deliver high frequency (typically 11-30 Hz) pressure bursts to provide an effective intrapulmonary percussion treatment. The high frequency pressure bursts are identical to those delivered by a high fre- quency ventilator.
The bursts or boluses of gas serve to mobilize secretions by creating a gasbolus velocity profile that travels down the center of the bronchial airways(Figure 1). This causes escaping or exhaled gas to travel at high speedsalong the wall of the bronchial airways imparting a sizeable force on bronchialsecretions moving them up and out of the airways.
The P-NEB is designed to oscillateduring inhalation for better aerosol
help increase the speed of gas alongthe walls of the bronchial airways. The pressure bursts also serve tointermittently squeeze the lymphsystem within the lung increasingthe flow rate at which fluids areprocessed through the lymph sys-
P-NEB User’s Guide Functional and Operational Characteristics OPERATIONAL CHARACTERISTICS
Suitable patient body weight . Greater than 10 kgTypical percussive oscillation frequency . Up to 30 Hz (1800 per minute)Device flow . 43 to 73 L/minFractional inspired Oxygen (FiO ) . Greater than 80% when
Operating environmental limits . 5 to 40° CStorage environmental limits . -20 to 60° CPatient connection . MouthpieceGas inlet . DISS connectionNebulizer reservoir size . 20 mLApproximate dimensions . 10" x 8" x 3.5"Approximate weight . About 190 grams
Clinical Considerations
The P-NEB is intended to be used only on those patients who are able tobreathe spontaneously. The P-NEB is intended to be used with the attachedmouthpiece. If a corrugated tube is connected between the mouthpiece andthe patient, the pressure bursts received by the patient would be muchweaker and dramatically less effective.
The P-NEB requires some coordination and training. On inhalation, the pa-tient should be encouraged to inhale as deeply as possible. On exhalation,the patient should be encouraged to exhale slowly and for as long as possible. Because the pressure bursts provide some measure of ventilatory support,patients will usually be comfortable exhaling for longer period of time. Ini-tially, some patients may be tense so the P-NEB may not oscillate as desired. However, as the patient relaxes during exhalation, the P-NEB will be able tofunction properly. Every patient is different so adjustment of flow and pres-sure settings, training, and good clinical judgment are all important. Some patients will allow their cheeks to puff out with each pressure burst ofthe P-NEB. This should be strongly discouraged because it reduces the pres-sure effect reaching the lungs.
The P-NEB nebulizer may be filled with up to 20 mL of liquid. Physiciansshould select medication carefully to achieve optimal benefits. In any event,it is important that the patient receives moisture during the treatment. P-NEB User’s Guide Clinical Considerations (continued)
The P-NEB nebulizer has an output during inhalation of approximately 1 mL/
min which depends on the patient’s inhalation efforts. It is recommended
that the P-NEB reservoir be filled with 1 mL of inhlation solution for every
minute of aerosol treatment. Because on exhalation, when the patient
should not be receiving any aerosol, the output is much less. Therefore, the
average output during the entire treatment will be less than 1 mL/min. Using
20 mL in the nebulizer reservoir, there will generally be residual liquid left
The gas flow required to operate the P-NEB is typically about 60 L/min. This
depends on the patient and the frequency desired. Generally, more airflow
will increase the frequency. The most common flowmeters are 15~16 L/min
float type flowmeters (Timeter, Puritan Bennett, etc.). When these
flowmeters are opened all the way, the float (ball) appears to ride just above
the 15~16 L/min mark but in fact is delivering a much higher flow when
connected to a P-NEB. In general, the clinician may vary the flow to what-
ever value is desired. If the P-NEB is oscillating primarily during exhalation
at an acceptable frequency, then the P-NEB is receiving the appropriate flow.
The PercussiveNEB improvements in ease of use, durability, dependability,
and performance attributes has resulted in a device that is more user
friendly, reliable, and is adjustable to patient needs. The PercussiveNEB’s
pressure dial allows users to set airway pressure oscillation amplitude for
individual comfort. It is also quieter, able to oscillate over a wider frequency
& pressure range, and is easier to operate within the source flow range. The
P-NEB User’s Guide Clinical Considerations (continued)
The percent time a positive pressure burst is being delivered to the patient
per oscillation is 25-33%. This is equivalent to an I:E ratio ranging from 1:3
to 1:2. This ratio is important because it allows sufficient time for lung and
lymph tissue to return to its resting state between pressure bursts.
The volume of gas delivered per pressure burst ranges from 35 to 75 mL,
depending on frequency and flow rate. The pneumatic capacitor is designed
to prevent more then 75 mL per pressure burst, regardless of the patient or
When using medication with the P-NEB Nebulizer, the clinician should first add
the desired medication to the reservoir and then top off to 15 to 20 mL by
adding the necessary volume of saline or respiratory quality water. Treat-
ment times are typically 15 to 20 minutes.
It is important when reassembling the P-NEB to screw the nebulizer cap on
securely and press the modulator into place firmly. If large leaks exist the P-
The P-NEB may be used with compressed air or oxygen. The P-NEB may be
cleaned by washing with mild soap (detergent) followed by rinsing with water
and allowing to air dry (see instructions). Nebulizer Top Modulator Mouthpiece Nebulizer reservoir (with Amplitude baffle inside) P-NEB User’s Guide III. Protocol: Setup Instructions - PercussiveNEB (HIGH FREQUENCY INTRAPULMONARY PERCUSSIVE NEBULIZER)
Use of the intrapulmonary percussive nebulizer in an acute care hospi-
tal setting. This policy is intended for patients meeting clinical indica-
tions for use of the percussive device. This policy is further intended
for use by licensed hospital personnel trained in the use of aerosol/
pressure delivery devices. This policy is applicable only upon individual
physician order, or with established medical staff approved clinical
protocols. For additional information, refer to the manufacturer’s oper-
To provide clinically appropriate recommendations for the use of the P-
NEB device, including clinical indications, device set-up, bedside appli-
cation, potential hazards, and documentation. Clinical Logic (New Device Policy)
Intrapulmonary Percussive Ventilation is a form of physical therapy,
administered to the Pulmonary Airways by a pneumatic device called a
“High Frequency Intrapulmonary Percussive Device” (PercussiveNEB).
The patient breathes through a mouthpiece which delivers preset
driving pressure and frequency. The PercussiveNEB automatically
triggers during exhalation to provide intrapulmonary percussion at 11
to 30 Hz (660 to 1800 cycles per minute). The PercussiveNEB delivers
PEEP at 2 to 8 cm H O, aerosol rate during inhalation of 1 mL/min, with
aerosol particle size distribution of 2 to 4 mm MMAD. During the per-
cussive bursts of air into the lungs, a continued wedge pressure is
maintained, while a high velocity inflow opens airways and enhances
endobronchial secretion mobilization. Moreover, the P-NEB is a dispos-
able unit that is useful in such areas as Isolation and Nuclear Medicine. P-NEB User’s Guide Protocol: P-NEB (continued) Procedure
Mobilization of retained endobronchial secretions
Contraindications
5.1.2 acute or high potential of pulmonary hemorrhage
5.1.3 not for patients receiving continuous ventilation
5.2.3 cardiovascular insufficiency (reduces coronary perfusion)
Effective therapy is accompanied by potential risks. The thera-
pist must be sensitive to potential hazards that may be recog-
nized early and prevented. IPV therapy should normally be
discontinued when the patient has received the optimum thera-
peutic benefit, or when the patient has become fatigued or has
requested discontinuation. Therapy must be discontinued if
there is any equipment malfunction, and the physician called
immediately if any complications arise.
Intrapulmonary percussive ventilation treatment will be immedi-
ately discontinued and the physician immediately contacted if
the patient demonstrates any of (but not limited to) the follow-
6.2.3 any sign of hypertension or hypotension
6.2.5 any indication of allergic reaction to the medicine, diluent,
P-NEB User’s Guide III. Protocol: P-NEB (continued)
6.2.6 increased HR > 20 beats/min from baseline value
6.2.7 decreased SpO < 92%, or increasing FI O requirement with
6.2.9 increase in abdominal distention or discomfort
6.2.10any unexpected increase in hemoptysis
6.2.11onset of dysrhythmia during therapy
6.3.2 Nippled oxygen tubing (comes with device)
6.4.1 Remove PercussiveNEB from packaging.
6.4.2 Place prescribed amount of medication into nebulizer and dilute
with saline to obtain desired total volume of liquid.
NOTE:The aerosol output of the PercussiveNEB is dependent on the
patient’s breathing pattern. The patient entrains air through the
nebulizer during inhalation allowing for the maximum dose of
medication. There should be 1 mL of fluid in the nebulizer reser-
voir for approximately every 1 minute of treatment. (NEBULIZER
P-NEB User’s Guide III. Protocol: P-NEB (continued)
6.6.1 Explain the purpose and rationale to the patient/family prior to
initiating treatment. Continue to assess/supplement the
patient’s understanding of the therapy at subsequent treat-
6.6.2 Position the patient in an upright, comfortable position, and
provide appropriate supplemental O as indicated to keep Sp O
6.6.3 Patient pre-treatment assessment will include full “Respiratory
Care Assessment” with subsequent reassessment q day.
6.7.1 Perform a FUNCTIONAL CHECK by occluding the mouthpiece
and adjusting flow until oscillation begins. Patients will require
DO NOT use if device fails to oscillate.
The normal flow rate for PercussiveNEB is 60 L/min
(+ 25%). The majority of the flow is used for operating the
internal components and is not delivered to the patient.
6.7.2 Place the mouthpiece in patient's mouth. Instruct the patient to
breathe through the mouth, not the nose. Best results are
achieved when the patient is relaxed and breathing normally.
The PercussiveNEB will oscillate during exhalation and inhala-
6.7.3 Adjust flow rate as required until the modulator piston is heard
or seen to be oscillating during exhalation. For best results,
adjust the flow to accommodate patient's comfort and breathing
ADJUST FLOW RATE P-NEB User’s Guide III. Protocol: P-NEB (continued)
6.7.4 Adjust oscillating amplitude as needed for patient's comfort and
percussine effects. For best results, start at SOFT setting and
gradually increase to HARD setting to accommodate patient's
Positive End Expiratory Pressure (PEEP) is intrinsic to this
device. Baseline pressure can reach up to 8 cm H O. ADJUST AMPLITUDE ENLARGED
6.9.1 Airway clearance therapy will be documented in the appropriate
area; i.e. Golden Rod or Phamis charting system, and will in-
Therapeutic objectives, tolerance, benefits, and ad-
HR, RR, and B/S (before, during, and after).
Cough evaluation/secretion clearance (amount, color,
6.9.2 Billing – billing will be done according to standard regional car-
diopulmonary billing procedures for airway clearance therapy. P-NEB User’s Guide III. Protocol: P-NEB (continued)
6.10.1 The PercussiveNEB is intended to be used on a single patient
6.10.2.1 Remove modulator from main column.
6.10.2.2 Rotate nebulizer top counterclockwise ¼ turn and lift
6.10.2.3 Remove baffle from reservoir.
6.10.2.4 Wash all components using soapy water (detergent)
and rinse throughly after every treatment. Cleaning Assembly
6.10.3.1 Reassemble in the reverse order of Steps 1 through 3.
6.10.3.2 Make sure all components are firmly in place.
6.10.3.3 The PercussiveNEB is now ready to use. Nebulizer Top Modulator Mouthpiece Nebulizer Amplitude reservoir (with baffle P-NEB User’s Guide Cautions and Warnings Cautions
1. Positive End Expiratory Pressure (PEEP) is intrinsic to this device.
Typical baseline pressure can reach up to 8 cm H O.
2. To be used only by persons having adequate training. Warnings
Not for patients receiving continuous ventilation. P-NEB User’s Guide P-NEB Competency
How to set up and use the PercussiveNEB - a new and unique single patientintrapulmonary percussive ventilation device used for clearing endobronchialsecretions from patients’ airways. Objectives
To be able to set up, clean and care for the PercussiveNEB andknow the optimal flow setting and gas source requirements.
To understand the mechanism of intrapulmonary percussionventilation - frequency (11 to 30 Hz) and pressure amplitude(PIP and PEP).
To know the characteristics of the aerosol components(medication and saline) of the PercussiveNEB. Troubleshooting the PercussiveNEB
1. The flow is the only power source for the PercussiveNEB. Higher flow
means more percussive effect and higher frequency.
2. If the nebulizer has an output of 1 mL/min and there is still liquid in the
reservoir after a 20-minute treatment, should all the liquid be gone?
After completion of the PercussiveNEB competency, the Respiratory CarePractitioner should be able to set up the PercussiveNEB and troubleshootproblems that may arise during its use. P-NEB User’s Guide FAQ (Frequently Asked Questions) Question
No, this is not a problem. It occurs when ad-
justing the flow to a setting that produces a high
The flow rate is set too high. Reduce the flow.
If you are connected directly to a 50 PSIG
source, you will have to use a flow meter or a
It is important to assemble the PecussiveNEB
tightly. If a large leak is present, it will not work
as well. This is particularly important after
cleaning. Be sure the nebulizer cap is screwed
on tightly and that the modulator has been
pushed firmly into place. Lastly, ensure that you
It depends. As long as the PercussiveNEB is
cycling during exhalation at a rate appropriate
for clearance and is well tolerated by the patient,
then the flow is acceptable. If not, a flow meter
All float/ball type 15 L/min flowmeters tested by
VORTRAN Medical Technology 1 will provide
sufficient flow when dialed all the way open.
Under such circumstances the ball indicates a
flow only slightly higher then 15 L/min, but it is
actually delivering a lot more flow.
No. Compressors designed for small volume
nebulizer treatments are not capable of deliver-
ing the needed flow. Most hospital equipment
rental agencies rent compressors large enough
to power a ventilator. This is needed for the
PercussiveNEB. You will also probably want to
equip the compressor with a flow meter. P-NEB User’s Guide FAQ (continued) Question
A physician must prescribe the type of medica-
tion and the amount for each treatment. Com-
monly used medications are Beta agonists,
anticholinergics, and mucolytics. To mix the
medication, first place the prescribed amount of
medication into the nebulizer reservoir. Then
add saline or respiratory quality water to make a
The nebulizer has an output of 1 mL/min during
inhalation when the patient is actually receiving
aerosol. During exhalation the output of the
nebulizer is less so it is normal to have liquid left
over in the reservoir. Actual outputs will vary
with each patient. It is important that liquid is
present in the nebulizer reservoir during the
The PercussiveNEB is single patient, multiple
Under normal operating condition, your device
should last about 100 hours of operation. If you
do two - 15 minutes per day, it will last about 90
P-NEB User’s Guide VII. Clinical Reference
RL Chatburn; HIGH-FREQUENCY ASSISTED AIRWAY CLEARANCE, Respiratory Care 2007;52(9):1224–1235. Summary High-frequency airway clearance assist devices generate either positive or negative transrespiratory pressure excursions to produce high-frequency, small-volume oscillations in the airways. Intrapulmonary percussive ventilation creates a positive transrespiratory pressure by injecting short, rapid inspiratory flow pulses into the airway opening and relies on chest wall elastic recoil for passive exhalation. High-frequency chest wall compression generates a negative transrespiratory pressure by compressing the chest externally to cause short, rapid expiratory flow pulses, and relies on chest wall elastic recoil to return the lungs to functional residual capacity. High-frequency chest wall oscillation uses a chest cuirass to generate biphasic changes in transrespiratory pressure. In any case (positive or negative pressure pulses or both), the general idea is get air behind secretions and move them toward the larger airways, where they can be coughed up and expectorated. These techniques have become ubiquitous enough to constitute a standard of care. Yet, despite over 20 years of research, clinical evidence of efficacy for them is still lacking. Indeed, there is insufficient evidence to support the use of any single airway clearance technique, let alone judge any one of them superior. Aside from patient preference and capability, cost-effectiveness studies based on existing clinical data are necessary to determine when a given technique is most practical. Key words: high frequency, airway clearance, secretion removal, intrapulmonary percussive ventilation, high-frequency chest wall compression, high-frequency chest wall oscillation. [Respir Care 2007;52(9):1224–1235. 2007 Daedalus Enterprises] Robert L Chatburn RRT-NPS FAARC is affiliated with the Section of Respiratory Care, Cleveland Clinic, Cleveland, Ohio, and with the Department of Medicine, Lerner College of Medicine, Case Western Reserve University, Cleveland, Ohio.
PILOT STUDY:PERCUSSIVE NEBULIZER VS. TRADITIONAL BRONCHIAL HYGIENE THERAPYFOR TREATMENT OF POST OPERATIVE ATELECTSIS IN CARDIAC SURGERY PATIENTSJohn Garcia, RRT, Kasem Loui, RRT, NPS, Luis Moreta-Sainz, MD. Kaiser Permanente Los AngelesMedical Center, Los Angeles, CA. Presented at 50th AARC International Rspiratory Congress in NewOrleans, LA., Dec 4-7, 2004BACKGROUND: Kaiser Permanente Los Angeles Medical Center is the regional tertiary care center forcardiac surgery. A well known complication of cardiac surgery is post-operative atelectasis. The traditionalbronchial hygiene therapy approach to post-operative atelectasis includes intermittent positive pressurebreathing (IPPB) treatments followed by chest physiotherapy (CPT). Traditional therapy is extremely laborintensive and has in our experience demonstrated marginal clinical efficacy. Moreover, the traditionalbronchial approaches to post-operative atelectasis are inconsistent with our evidence based practice model. Therefore a pilot study was conducted utilizing a disposable single patient use percussive nebulizer (PN). METHOD: 26 post-operative cardiac surgery patients who met our treatment criteria for post-operativeatelectasis were placed on PN therapy and evaluated: Our treatment criteria for both groups included:increasing fiO requirements, ABG demonstrating hypoxemia and/or hypercarbia with or without acidosis,
and chest x-rays (CXR) showing atelectasis or infiltrates. Clinical improvement was defined as: clearing orimproved CXR, and a decreasing fiO requirement with an average fiO of .25 and SpO of 96%. RESULTS:
All 26 patients in the PN group presented with atelectasis on CXR and were receiving high levels supplemen-tal oxygen with an average fiO of .60 pre PN therapy. Of these patients, 24 showed clinical improvement in
an average of 3 days. There were two PN treatment failures, one due to late intervention and another due tocardiac failure. Both patients required reintubation and mechanical ventilation. EXPERIENCE: PN appearsto be a viable alternative to our traditional bronchial hygiene regimen though a more thorough investigationshould be undertaken. CONCLUSIONS: Treatment of atelectasis in post-operative cardiac surgery patientswith PN appears to be a more effective and efficient use of departmental resources than traditional bronchialhygiene procedures. P-NEB User’s Guide VII. Clinical Reference (continued)
Finder, Jonathan MD; Airway Clearance Techniques - Trends in the Treatment of Lung Diseases, Respiratory Magazine, Issue: November 2007.
CPT has been the standard for CF care since the 1960s, but newer techniques are finding acceptance, too. In respiratory medicine, one constant theme is the importance of airway clearance in maintaining health. Airway (secretion) clearance consists of two linked systems: mucociliary clearance and cough clearance. Oscillation Devices
High-frequency chest-wall oscillation (CWO), as a term, should not be used interchangeably with HFCC. High-frequency CWO refers to the Hayek Oscillator™ (Breasy Medical Equipment, Charlotte, NC), whichis a negative-pressure ventilator that uses a cuirass interface around the chest. Just one study 15 using thisdevice in CF has been published, and the authors found that it was not as effective as techniques using theactive cycle of breathing; they concluded that high-frequency CWO was not an effective airway-clearancemodality in CF exacerbations. Just as HFCC oscillates the air within the lung, handheld devices thatoscillate a column of air within the airway help to shear secretions away from the wall of the airway and helpmobilize them for expectoration. They are similar in function to HFCC. One difference, though, is thathandheld oral airway oscillators generally provide some positive airway pressure to help maintain airwaypatency during breathing. Therefore, they are often discussed in the context of PEP. The first reports16 onoral airway oscillation demonstrated an increase in expectorated sputum volume, compared with conven-tional CPT. The original device (Flutter, Axcan Pharma, Birmingham, Ala) used a metal ball that oscillatedbased on gravity, and therefore was quite positionally sensitive. Later devices used magnetic attraction toopen and close the valve (Acapella, Smiths Medical, Waukesha, Wis) or a hand-cranked mechanism to openand close a valve (Quake, Thayer Medical Corp, Tucson, Ariz), thereby rapidly opening and closing theairway’s opening during expiration. The hand-cranked device also has the advantage of allowing airwayoscillation during the inspiratory phase, and it does not rely on a high flow rate for function. This device maybe more useful in patients with more severe obstructive defects. No head-to-head studies of these deviceshave ever been performed. Two other devices, which were designed for hospital use, also deliver nebulizedmedications via positive, oscillating pressure: the PercussiveNEB® (Vortran, Sacramento, Calif) andintrapulmonary percussive ventilation (IPV®, Percussionaire, Sandpoint, Idaho). The PercussiveNEB hasnot been shown to be effective, and its use remains limited. IPV uses small, rapid, high-flow bursts of air tohelp loosen secretions; it has been studied17,18in patients with neuromuscular weakness and atelectasis. Anecdotal reports have indicated that IPV is a useful adjunct in clearing atelectasis in patients with neuro-muscular weakness. IPV has also been evaluated19 in CF in comparison with the Flutter and CPT. Nodifferences were found, suggesting that IPV is no less effective than other forms of airway clearance. IPVwas also well tolerated. The largest study group consisted of 16 subjects, limiting, to some degree, theusefulness of this work. Despite these promising reports from the mid 1990s, no larger follow-up studieshave been published.
Jonathan Finder, MD, is associate professor of pediatrics, University of Pittsburgh. P-NEB User’s Guide VII. Clinical Reference (continued) PercussiveNEB™ (P-NEB) COST COMPARISON Estimated Cost (Daily - Based on QID) Cost - 1 day BENEFITS COMPARISON
PULMONARY FUNCTION AND SPUTUM PRODUCTION IN PATIENTS WITH CYSTIC FIBROSIS* A PILOT STUDY COMPARING THE PERCUSSIVETECH HF DEVICE AND STANDARD CHEST PHYSIOTHERAPY. John H. Marks, MD, FCCP; Karyl L. Hare, RN, CDE; Robert A. Saunders, RRT and Douglas N. Homnick, MD, MPH, FCCP, et al. American College of Chest Physicians Chest. 2004;125:1507-1511.* From the Pediatric Pulmonary Division, Department of Pediatrics, Michigan State University, Kalamazoo Center for Medical Studies (Drs. Marks and Homnick, and Ms. Hare), and Pulmo- nary Function Laboratory, Bronson Methodist Hospital (Mr. Saunders), Kalamazoo, MI. Study objective: To compare the PercussiveTech HF (PTHF) device (Vortran Medical Technology 1; Sacramento, CA) to standard manual chest physiotherapy (CPT) with respect to acute changes in pulmonary function, sputum production, and pulse oximetry in patients with cystic fibrosis (CF). Design: Randomized crossover. Setting: University-affiliated, community-based CF center. Participants: Ten clinically stable patients with CF (age range, 10 to 21 years; mean age, 15.3 years) with Shwachman scores from 55 to 95 (mean 75). Interventions: Two treatment regimens were used: 2.5 mg of albuterol delivered via updraft nebulizer followed by standard CPT, and 2.5 mg of albuterol delivered via the PTHF device without CPT. Results: Outcome measures included pulmonary function test (PFT) results 4 h after treatment and quantita- tive sputum production during the 4 h after treatment. Pulse oximetry was performed during treatment. A patient satisfaction questionnaire was administered at the end of the study. No PFT parameters were significantly changed 4 h after CPT or PTHF, although there was a trend to decreasing residual volume after both treatments. There was a trend for more sputum production after PTHF compared to CPT, but this did not reach statistical significance. There were no episodes of hemoglobin-oxygen desaturation during or after either treatment. One patient had minor hemoptysis after CPT. No adverse effects occurred after PTHF. Eight patients found the PTHF device easy to use, and six patients would prefer the PTHF device to CPT. Conclusions: The PTHF device appears to be a safe and effective method of airway clearance in CF patients in this small pilot study. P-NEB User’s Guide VII. Clinical Reference (continued) J. H. Marks; D. N. Homnick; K. Hare; D. Cucos; THE PERCUSSIVETECH HF COMPARED TO THE FLUTTER DEVICE IN CYSTIC FIBROSIS PATIENTS: A SIX MONTH PILOT STUDY, Presented at 2001 North American Cystic Fibrosis Conference, Orlando World Center Marriott, Orlando, Florida, Oct 25-28, 2001.
Airway clearance devices, such as the Flutter or Intrapulmonary Percussive Ventilator, are acceptedairway clearance methods for CF patients. The PercussiveTech-HF(PTHF) is an intrapulmonarypercussive treatment device that also delivers a large volume (20ml) aerosol. The PTHF oscillatesprimarily during exhalation providing intrapulmonary percussion at 6 to 14 Hz with positive expiratorypressure of 10-20 cm H2O. In a pilot study of the PTHF device we showed safety and effectivenesscompared to standard chest physiotherapy.*Aims: This study compared the longterm effects of twice-daily use of the PTHF device with the Flutterdevice in patients with CF. Outcome measures included FEV1(primary), FVC, FEF25-75, number ofdays of hospitalization, lost school or work, and IV antibiotic use. A patient satisfaction questionnairewas given to the PTHF group. Methods: Sixteen patients were randomized to either Flutter (3F, 5M) orthe PTHF (4F, 4M). At enrollment spirometry and Shwachman score were obtained. All subjects thencompleted one week of twice-daily Flutter treatments. After day 7 baseline spirometry was obtained,the PTHF group started twice-daily treatments while the Flutter group continued twice-daily Fluttertreatments. All patients received 2.5mg of albuterol in saline, 20ml in the PTHF group, and 3ml in theFlutter group, with each treatment. Spirometry was repeated every 4 weeks until the end of the study at24 weeks. Pulmonary exacerbations requiring hospitalization or home IV antibiotics were noted. PTHFquestionnaires were completed at each visit. Results: Fifteen patients completed the 24 week study, 8Flutter, 7 PTHF. One became pregnant and was excluded. Both groups had a similar mean age(95%confidence interval (CI)) Flutter 14.1(10.5;18), PTHF 10.9(8.4;13.3) and Shwachman score,Flutter 72.6(62;83), PTHF 79.6(68;91). There were no significant differences between groups at day 7baseline for mean per cent predicted FEV1 -Flutter 56% (41;71) and PTHF 75.6% (53;98) p=.208, orFVC- Flutter 78% (60;96), PTHF 90.6% (70;111), p=.292, or FEF25-75- Flutter 30% (16;44) andPTHF 58% (28;89), p=.0513. At week 24 there were no significant differences between groups inFEV1(p=.208), FVC(p=.292), or FEF25-75 (p=.126). Within groups there is no significant differencebetween baseline and week 24 for FEV1 - Flutter p=.98, PTHF p=.471, FVC- Flutter p=.717, or thePTHF group p=.149, or FEF25-75 - Flutter p=.697, PTHF p=.29. There were no differences betweengroups in the mean number of hospital or home IV antibiotic days. Patient satisfaction with the PTHFtreatments was good, with 67% of patients willing to continue using the PTHF instead of other airwayclearance methods. Conclusions: The PTHF device was well tolerated and generally well accepted as asan airway clearance method by CF patients in this 6 month pilot study. The PTHF may be as effectiveas the Flutter device, however, larger studies are needed to assure the long-term effectiveness.
*Marks JH, Homnick DN. Pediatr Pulmonol 1999; Suppl.19:290. Supported by Vortran Medical Technolog 1, Inc. P-NEB User’s Guide VII. Clinical Reference (continued)
Marks, John H 1, Hare KL1, Homnick DN1., PULMONARY FUNCTION AND SPUTUM PRODUC- TION IN PATIENTS WITH CYSTIC FIBROSIS: A PILOT STUDY COMPARING THE PERCUSSIVETECH HF DEVICE AND STANDARD CHEST PHYSIOTHERAPY, (1. Michigan State University, Kalamazoo Center for Medical Studies, Kalamazoo, MI, USA.), Accepted for presentation at 13th Annual North American Cystic Fibrosis Conference in Seattle, Washington, October 7- 10, 1999. Abstract: Manual chest physiotherapy with gravity assisted drainage (CPT) continues to be the standard method of airway clearance for patients with cystic fibrosis (CF). While CPT has long been shown to aid in clearance of pulmonary secretions in CF patients, compliance in the daily regimens of therapy are often an issue due to time involved and the need for assistance in such therapy. Several devices have been shown to be effective in aiding airway clearance in CF patients, including positive expiratory pressure (PEP), the flutter device, high frequency chest wall compression vest and the intrapulmonary percussive (IPV). We have previously reported on the effectiveness of the IPV com- pared to CPT and the flutter device. This study compares a new airway clearance device, the PercussiveTech HF (PTHF), with CPT in patients with CF. The PercussiveTech HF device delivers rapid, mini-bursts of air (intrapulmonary percussion) with high volume aerosol delivery. Ten clinically stable patients with CF (age 10 to 21 years) were randomized to receive PTHF or CPT regimens on one day with crossover to the alternate treatment one week later. Regimens included 2.5 mg albuterol in 2 cc NS by standard nebulizer followed by standard chest physiotherapy using CFF guidelines, or 2.5 mg albuterol in 15-20 cc NS by the PTHF device without CPT. Compressed air was used for the standard nebulizer and the PTHF and pulse oximetry was monitored during each treatment. Baseline pulmonary function (PFTs), including FVC, FEVI, FEF25-75, TLC, RV, were obtained prior to each treatment. Repeat PFTs were performed 4 hours after completing each regimen and sputum was collected over the 4 hour period. Sputum was collected with the use of cotton wool dental dams. Sputum wet and dry weights were measured. Nine participants completed the study. No PFT param- eters were significantly changed after CPT or PTHF, although there was a trend to decreasing RV after both therapies. There was a trend for more sputum production after PTHF compared to CPT, mean wet weight 13.72 gm vs 7.75 gm and dry weight 1.47 gm vs 0.51 gm, but this did not reach statistical significance. There were no adverse events during or after either therapy except for minor hemoptysis in one patient after CPT. Eight patients found the PTHF easy to use and six would prefer it over CPT.
Douglas N. Homnick, M.D., M.P.H.; Fred White, R.R.T.; and Carol de Castro, B.S., R.N.: Comparisonof Effects of an Intrapulmonary Percussive Ventilator to Standard Aerosol and Chest Physiotherapy inTreatment of Cystic Fibrosis, Pediatric Pulmonary, 1995, 20:50-55.
Summary: Impaired mucociliary clearance due to defective ion and water transport and the effects ofchronic airway infections lead to stasis of secretions and progressive pulmonary damage in patientswith cystic fibrosis (CF). Methods to improve removal of tenacious lung secretions in CF patientscontribute to slowing the decline in respiratory function. We have evaluated an intrapulmonarypercussive ventilator (IPV), which is a device designed to enhance airway clearance and preserve lungfunction. A previous pilot study by us had determined that the device was acceptable to patients and issafe. We undertook a 6 month parallel comparative trial of the IPV versus standard, manual chestphysiotherapy in 16 CF children and adults. No significant differences in spirometric measures,numbers of hospitalizations, use of oral or IV antibiotics, or anthropometric measurements weredetected between the standard aerosol chest physiotherapy group and the IPV group over the durationof the trial. Patient acceptance, as determined by participant survey, was good. The device appeared tobe safe and durable. It was concluded that the IPV is as effective as standard aerosol and chestphysiotherapy in preserving lung function and anthropometric measures, and there was no difference inthe use of antibiotics and hospitalizations. P-NEB User’s Guide VII. Clinical Reference (continued) COMPARISON OF AIRWAY PRESSURE AND OSCILLATION FREQUENCY OF FOUR AIRWAY CLEARANCE DEVICES
D. Blackney and B. ChippsCystic Fibrosis Center, Sutter Memorial Hospital, Sacramento, CA, USA
BACKGROUND: Factors that improve mucus clearance rate are important for patients with cystic fibrosis. Studies have shown that high frequency oscillation enhances tracheal mucus clearance. Comparison of airway pressure waveforms and oscillation frequency for four airway clearance devices was recorded to compare the operational characteristics of intrapulmonary percussion effects. METHODS: Each device was connected to a pressure transducer on the mouthpiece and pressure waveforms were recorded using a computer sampling at 300 Hz. Devices were operated by a trained respiratory care practitioner and pressure waveforms were recorded. RESULTS: The results of this evaluation are summarized below with pressure waveforms. Percussionaire IPV PercussiveTech HF PRESSURE (cm-H TIME (SEC) TIME (SEC) TIME (SEC) TIME (SEC) DISCUSSION: The results indicated that peak pressure for all devices ranged from 15 - 26 cm- H O depending on the devices, setting and patient exhalation effort. However, the pressure
amplitude varied greatly for devices using external gas source (8 - 17 cm-H O) vs. patient’s own
effort (2 - 7 cm-H O). The oscillation frequencies also vary greatly with these two classes of
CONCLUSIONS: These results suggest that patient’s own effort can generate high frequency airway oscillation, but very little pressure amplitude is generated. Devices with external gas source can generate significant pressure amplitude, which may be beneficial along with the high frequency airway oscillation.
Supported by VORTRAN Medical Technology 1, Inc.
Accepted for presentation at 13th Annual North American Cystic Fibrosis Conference in Seattle,Washington, October 7-10, 1999. P-NEB User’s Guide VII. Clinical Reference (continued) COMPARISON OF MINUTE VOLUME DELIVERED WITH HIGH FREQUENCY VENTI- LATION USING TWO AIRWAY CLEARANCE DEVICES David A. Blackney, RCP, RRT, Pulmonary Services, Sutter Children’s Center, Sacramento, CA, USA BACKGROUND: High frequency ventilation has been used in devices to create intrapulmonary percussive effects and promote airway clearance. Two percussive devices were evaluated, and the flow and volume waveform characteristics were compared for high frequency oscillation. The parameters important for intrapulmonary percussive type ventilation are: f - oscillation frequency (Hz), proximal PIP - Peak Inspiratory Pressure (cm-H O), OTV - Oscillatory Tidal Volumes (ml),
and MV - Minute Volume (Liters) during inhalation and exhalation. METHODS: Each device was connected to a pressure tap and a flow sensor proximal to the mouthpiece to record pressure and flow waveforms using a computer data acquisition system sampling pressure at 100 Hz. Model IPV®-1 (Percussionaire® Corp.) was operated at both 20 and 40 PSIG at “EASY” setting, and PercussiveTech HF™ (VORTRAN Medical Technology 1, Inc.) was operated at 35 PSIG (approximately 60 L/min device flow). A 50 PSIG compressed air source was used. A trained respiratory care practitioner operated the devices and recorded pressure waveforms. RESULTS: The results of this evaluation are summarized below with flow waveforms. TIME (SEC) TIME (SEC) TIME (SEC) DISCUSSION: The results indicate that oscillation frequencies vary slightly depending on the setting of the devices. The oscillation frequency f for the IPV®-1 was from 5 to 7 Hz and the PT-HF was at 11 Hz. The exhalation Minute Volume (MV
x f) delivered by the IPV®-1 was 62
to 66 liters per minute at various frequencies. In comparison, the PT-HF delivered about 40 liters per minute at higher frequencies. CONCLUSIONS: The flow waveform of the PT-HF is compatible to that of the IPV®-1. PIP is essentially the same with the PT-HF oscillating at higher frequencies and at a lower pressure. The MV
results suggest that patients were ventilated during the exhalation phase through the use of
high frequency oscillation. Further studies should be done to evaluate the impact of volume deliveredon patients during exhalation and on the effectiveness of airway clearance at various frequencies.
Supported by VORTRAN Medical Technology 1, Inc. Accepted for presentation at 45th AARC International Respiratory Congress in Las Vegas, Nevada,December 13-16, 1999. P-NEB User’s Guide VII. Clinical Reference (continued) In-vitro Comparison of the Operational Characteristics of the PercussiveTech HF™ and Percussionaire® IPV® SUMMARY: The aerosol output and particle size distribution for the PercussiveTech HF™ and Percussionaire® IPV® are essentially identical using three common inhalation solutions. The pressure waveforms show that the PT-HF oscillates at a higher frequency (6-14 Hz) than IPV which could improve secretion mobilization and clearance.1 High frequency chest wall oscillation (HFCWO) and intrapulmonary percussive ventilation (IPV) are as effective as chest physical therapy and postural drainage (CPT&PD) 2. INTRODUCTION: The quality (particle size distribution) and quantity (output concentration) of aerosol produced by both devices were measured to determine their operational characteristics. Pressure waveforms were recorded to demonstrate the peak airway pressure and oscillation frequency for both devices under simulated breathing conditions. METHOD: Aerosol output and particle size were tested by setting up a lung simulator with a compliance of 0.02 L/cm-H O, a resistance of 20 cm-H O/L/sec, and a simulated inhalation flow of 25 L/min. Three
inhalation solutions [normal saline (0.9%), albuterol sulfate (2.5 mg), and metaproterenol sulfate (10 mg)]were selected for testing. The devices were run at two pressure settings (20 and 35 PSIG) for a total of 15minutes to simulate one treatment. Inhalation aerosol was sampled with a cascade impactor at 1.4 L/min for 2minutes at the beginning and end of the treatment for each test. The sample from the cascade impactor wasused to determine the amount of drug delivered and the particle size distributed in MMAD (mm) and GSD(s ). Pressure waveforms were recorded using a computer pressure and flow data acquisition system. The
patient simulator was set to a breathing rate of approximately 8 breaths per minute (B.P.M.) with an I:E ratio of approximately 1:1. Inspiratory and expiratory flow ranged up to 50 L/min. RESULTS: The estimated aerosol output delivered to the patient was essentially identical for both devices as measured under the simulated breathing conditions (I:E ratio of 1:1). The actual liquid consumption rate of the devices were about 1 mL/min.
The particle size distribution (MMAD and GSD) sampled over the duration of operation was essentially thesame for all three drugs delivered in mL/min. There was no significant difference in the aerosol outputcharacteristics for the new device (PercussiveTech HF) compared to the predicate device (PercussionaireIPV) in all modes of operation (20 or 35 PSIG, hard and easy settings). Particle Size Distribution
The pressure waveforms as recorded indicated that PT-HF is capable of cycling at a higher oscillatingfrequency than IPV. The peak pressure for PT-HF should not exceed 20 cm-H O when properly operated
while IPV was measured at up to 25 cm-H O. Pressure waveforms CONCLUSIONS: In-vitro testing of aerosol characteristics comparing the PercussiveTech HF and the Percussionaire IPV shows that the devices provide patients with equivalent aerosol quantity and quality and are, therefore, substantially equivalent. REFERENCE: 1. M. King, D. M. Phillips, D. Gross, V. Vartian, H. K. Chang, and A. Zidulka: Enhanced Tracheal Mucus Clearance with High Frequency Chest Wall Compression, American Review of Respiratory Diseases 1983, 128:511-515. 2. Castile, R, Tice, J., Flucke, R., Filbrun, D., Varekojis, S. and McCoy, K.: Comparison of Three Sputum Clearance Methods in In- patients with Cystic Fibrosis, abstract # 443 presented in 20th Annual North American Cystic Fibrosis Conference.
PercussiveTech HF™ is a trademark of VORTRAN Medical Technology 1, Inc. Percussionaire® and IPV® are registered trademarks of PERCUSSIONAIRE CORPORATION
P-NEB User’s Guide VIII. Coding information HCPCS - HCFA (Health Care Financing Administration) Common Procedure Coding System
PRODUCT --------- PercussiveNEB and Hi-Flow 70 Compressor
CODE -------------- E0481
DESCRIPTION----- Intrapulmonary percussive ventilation system
INSTRUCTIONS --- The SADMERC and the four Durable Medical
Equipment Regional Carriers (DMERCs) have completed the HCPCS Coding Verification Review on August 21, 2002. The PercussiveNEB and Hi-Flow 70 Compressor meets the characteristics and description of the HCPCS code as assigned for Medicare billing. CMS - CENTERS FOR MEDICARE & MEDICAID SERVICES CPT - Current Procedure Terminology (American Medical Association)
DESCRIPTION----- Manipulation chest wall, such as cupping,
percussing, and vibration to facilitate lung function;
initial demonstration and/or evaluation. P-NEB User’s Guide Troubleshooting Cause / Action
1. Leak in connection / look for pressure
2. Not enough flow / increase flow or change
closed position, puch open and clean.
2. Low on solution / need 3 to 5mL solution
1. Too much flow / reduce flow2. Amplitude too high / adjust pressure
amplitude dial out for lower amplitudepercussion.
1. Not enough flow / increase flow2. Amplitude too low / adjust pressure
amplitude dial in for higher amplitudepercussion. Ordering Information Accessories P-NEB User’s Guide Quick Guide
1 Add medication
the baffle is in place. Place 1 mL solution
mL in 20 minutes with 3-5 mL of residual.
2 Connect tubing
3 Set desired flow
4 Begin patient treatment and
Step 4 - Instruct the patient to create a seal around the
mouthpiece and breathe through the mouth, not the nose.
The P-NEB will cycle during inhalation and exhalation.
5 Adjust amplitude and flow for the desired frequency Step 5 - Adjust the amplitude ENLARGED VIEW
This Quick Guide is intended to help you gain a general understanding of the PercussiveNEB product. Pleasebe certain to read, understand, and follow the information listed in this User’s Guide before using this product.
2008 - VORTRAN Medical Technology 1, Inc., Sacramento, California U.S.A.
APPROVAL DATE EFFECTIVE DATE REVISION 05/01/11 INTRODUCTION Prior to commencing work involving carcinogens, chemotherapeutics or other hazardous drugs, the Principal Investigator must perform a hazard assessment in order to identify the proper personal protective equipment (PPE) and engineering requirements for handling hazardous compounds. A key element of the risk
Dr. Hans-Michael Hackenberg - Otitis externafile:///D:/Michas%20Daten/Webseiten/Site2005/pdf/tm3_pdf.htm Otitis externa (OE) - das gemeine Taucherohr Es gibt kaum ein Taucherleiden, das einem den Tauchurlaub so nachhaltig verderben kann wie dieEntzündung des äußeres Gehörganges. Wer jemals so ein „Taucherohr“ miterlebt hat, wird künftig allesdaran setzen, derartigem Leid vorzubeug

 USER’S GUIDEP-NEB User’s Guide
USER’S GUIDEP-NEB User’s Guide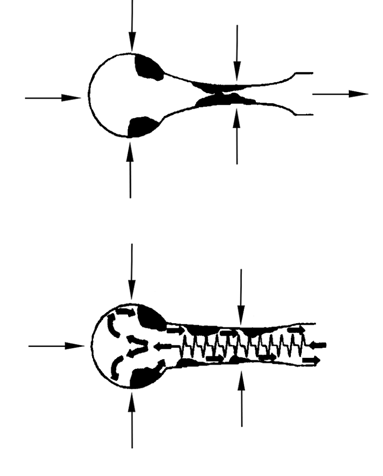 P-NEB User’s Guide
P-NEB User’s Guide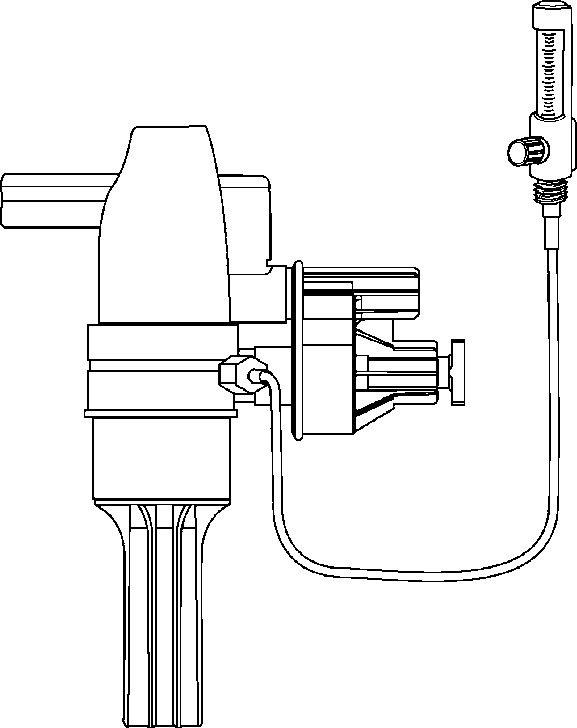 P-NEB User’s Guide
P-NEB User’s Guide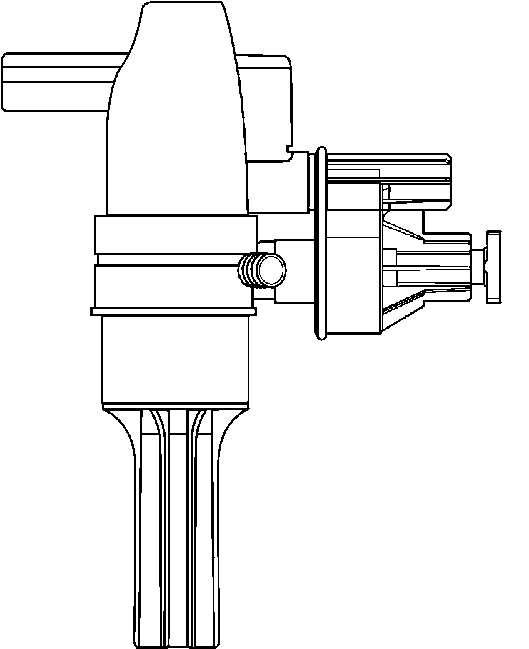 P-NEB User’s Guide
P-NEB User’s Guide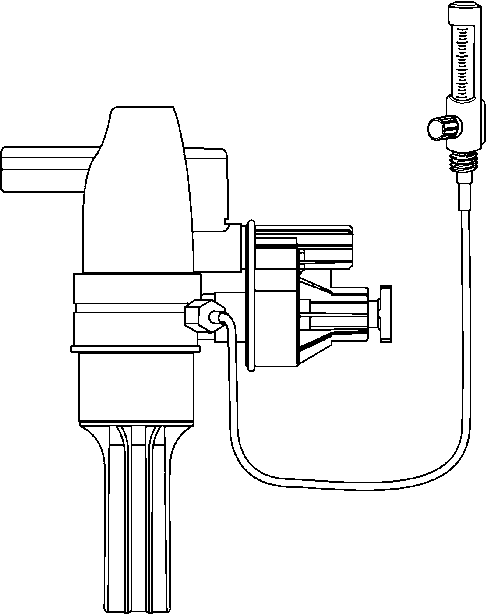 P-NEB User’s Guide
P-NEB User’s Guide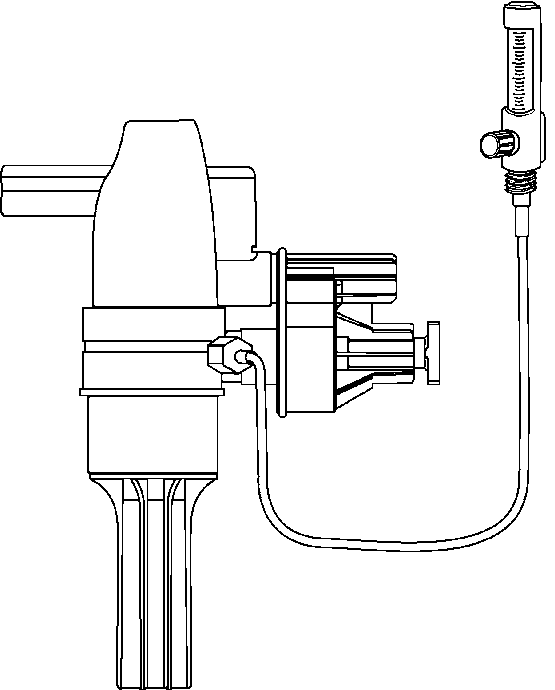

 P-NEB User’s Guide
P-NEB User’s Guide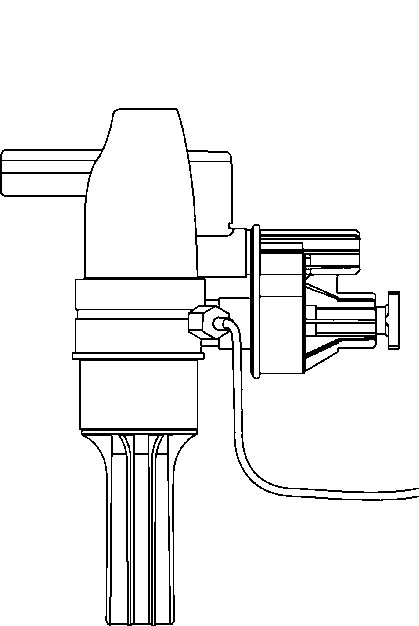
 P-NEB User’s Guide
P-NEB User’s Guide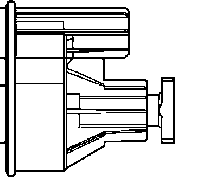
 P-NEB User’s Guide
P-NEB User’s Guide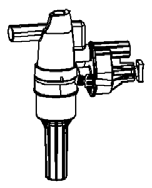 P-NEB User’s Guide
P-NEB User’s Guide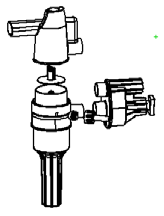
 P-NEB User’s Guide
P-NEB User’s Guide