Glossary
ORIF – Open reduction internal fixation
THJR/THR – Total hip joint replacement
TKJR/TKR – Total knee joint replacement
TAQ’s – Toe’s, Ankle’s, Quad’s exercises
Quads Lag – Able to extend knee but falls into a degree in flexion on SLR or IRQ
Quads Lack – Pt unable to fully extend knee and remains in this degree of flexion during
Useful reading!
David J. Dandy – Essential Orthopaedics and Trauma (616.7 DAN)
T. Duckworth – Orthopaedics and Fractures (616.7 DUC)
McRae and Kinninmonth – Orthopaedics and Trauma (616.7 MACR)
Analgesia Anti Emetic Subjective Examination
The subjective examination can mostly be taken from the patients notes and usually
briefer than one in an out patient setting. This is due to the fact that the patient has
already been referred for a joint replacement. The main aim of a pre-op assessment is to
find out the length of time the patient has had this complaint, present mobility status and
ROM (active and passive). This gives an indication of muscle shortening, altered gait or
need of a walking aid and any capsular pattern. During this the physiotherapist should
also ask about any previous joint replacements and the success of it.
PC – Constant pain and loss of function.
HPC – How long they have had present complaint,
DH – Analgesia and any other medication
Stairs and how many, bed and bath on same level.
Objective Examination of the HIP Active and passive ROM Muscle Power (Grade I-V) Alignment Test
Leg length discrepancy – The test is performed with the patient lying supine, with hips in
line and as flat as possible. Measurement is taken from the ASIS to the medial
malleolus on both sides. A difference signifies a leg length discrepancy.
Special tests
Thomas Test – This test is to rule out of confirm a hip flexion contracture. The test is
performed with the patient lying supine on the plinth. One knee brought to chest
and the other straight. Make sure the lower region of the lumbar spine remains
Ely’s Test – To assess for tightness of the rectus femoris. It is performed with the patient
lying supine with the knees hanging over the edge of the plinth. The unaffected
leg is brought to the chest stabilizing the pelvis and back. Extension of the test
Trendelenburg’s Test – To test pelvic stability maintained by the hip abductor muscles.
The patient stands on the test leg and raises the other off the floor. The test is
abnormal if the pelvis drops on the non-weight-bearing side.
Contraindications
• Twisting operated leg. The hip is put at risk if swivelled when turning,
• Bend the operated leg past 90°, bending to pick something off the floor when
seated or leaning forward from the waist.
• Avoid kneeling for the first four months.
Getting in and out of bed
1. Sit up and step legs towards edge of bed, operated leg must lead, as this reduces
the risk of operated leg passing mid line. For patients with a posterior incision
they must keep the knee of the operated leg straight and their trunk and operated
2. Sitting on the edge of the bed with unoperated foot flat on the floor and the other
3. Place hands on the bed at either side and push up to stand drawing the operated
leg back. When the patient is standing and well balanced, they should they take
GETTING BACK INTO BED IS THE REVERSE PROCEDURE OPERATED
Active/assisted, hip/knee extension only. No re-education boards.
These are only guidelines and therefore may alter if conditions changed. Post-op regime
for revision of total hip replacement will require modification and patient may require to
Teach deep breathing and circulatory exercises
Chest care i.e. deep breathing exercises
Commence active/ assisted hip/knee flexion/extension exercises either
Exercises as day one plus abduction exercises with re-education board
Depending on check x-ray or on doctors instruction, transfer out of bed and
Continue as day two but increase mobility
Encourage mobility with elbow crutches, stair practice with elbow crutches and
Patient can progress to two walking sticks or continue with elbow crutches
Outpatient follow-up only if required. Non-standard procedure
Guidelines for Total Knee Replacement
PoD 1 & PoD 2, patient may wear Buchanan splint (Monklands Hospital) until wound
checked and if satisfactory, then patient can commence knee flexion exercises. Patient
allowed to mobilise with splint in-situ. This can be discontinued once wound checked
and patient can SLR. At other sites, the post –op regime will vary and splints may not be
used. However, almost always, the check x-ray will be done before mobilising the
These are only guidelines and therefore may alter if conditions changed. Post-op regime
for revision of total knee replacement will require modification and patient may require
It can be very easy to become focused on the degree of knee flexion. This is easier to
achieve than knee extension, which is very important for gait. Remember to work on
extension too! A few examples are – long sitting or sup lye with a rolled up towel under
the ankle. This allows gravity to act on the knee, letting it stretch into extension. This can
be uncomfortable for the patient so use only for short periods throughout the day.
Another way to increase extension is to position the leg as above, with the ankle elevated
on a rolled up towel and passively stretch the knee into extension or perform SQ’s in this
Teach deep breathing and circulatory exercises
Chest care i.e. deep breathing exercises
Circulatory exercises – TAQ’s and gluts
Commence active/ assisted hip/knee flexion/extension exercises either
Depending on check x-ray or on doctors instruction, transfer out of bed and
Chair transfer and up to sit, leg usually elevated
Exercises as PoD 1, encourage active work and SLR
If patient not mobilised on PoD 1, patient usually mobilised PoD 2
If drain is removed and dressing reduced commence use of cryocuff or ice pack,
compression bandage (TED stockings) must be applied when cryocuff/ice pack
If not already progressed changed from ZWA to E/C or 2x walking sticks
Continue to evaluate and modify treeatment.
Continue modify and increase exercises i.e. modified PNF
Encourage mobility with elbow crutches/sticks, stair practice with elbow
crutches/sticks and rail or with elbow crutches/sticks only.
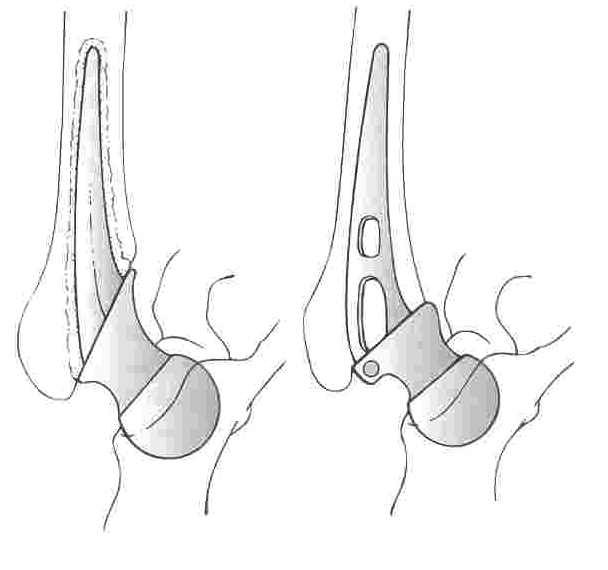
Types of hip replacements
The Thompson and the Austin-Moore hemiarthroplasties are the commonest types of hip
replacements used in the UK. The total hip replacement replaces the damaged head of
femur with a stainless steel ball mounted on a stem and relines the acetabulum with a
special plastic polyethylene socket. The components are usually attached to the bone
with a type of cement called Methyl Methacrylate, shown in figure A. Figure B shows a
prosthesis applied with no cement, the type of prosthesis used is to the discretion of the
215 Forest Park Circle Panama City, FL 32405 *Office 850-215-5657 CONFIDENTIAL SKIN HEALTH SURVEY Name: ____________________________ Date of Birth: ____/____/____ Intake Date: ____/____/_____ Address: _____________________________________ Your Occupation ______________________________ Emergency Contact-Name: ___________________________ Address: ____________________________________
CURRICULUM VITAE Nombre y Apellido: Diana Ester Fernández Calvo Estado Civil: casada Domicilio: Avellaneda 432 Capital (C.P.1405 ) Teléfono: 4903-4800 E-mail: [email protected] http://www.dcalvo.freeservers.com http://www.musicaclasicaargentina.com/tecnologia/index.htm c Fax: 4901-7710 Celular: 1551398188 TÍTULOS DE GRADO UNIVERSITARIO Licenciada en Música, especialidad Educaci�
 Types of hip replacements
Types of hip replacements