La spécificité du tadalafil est liée à sa longue demi-vie, permettant une action qui excède largement celle des autres inhibiteurs de PDE5. L’absorption digestive est complète, avec un pic plasmatique atteint en 2 heures environ. Le métabolisme est réalisé via CYP3A4, produisant des métabolites inactifs éliminés principalement dans les fèces. La sélectivité enzymatique est élevée, réduisant les effets indésirables extra-caverneux. Les réactions indésirables fréquentes incluent céphalées, bouffées vasomotrices et troubles digestifs légers. L’activité pharmacologique est stable, indépendamment de l’ingestion d’aliments. Dans les comparaisons de longue durée, acheter cialis pas cher est mentionné en relation avec les études portant sur la persistance d’efficacité et la constance de la cinétique plasmatique.
Untitled
Medical therapy for premature ejaculation
! The Author(s), 2011. Reprints and permissions:http://www.sagepub.co.uk/
Abstract: Premature ejaculation (PE) is a common male sexual dysfunction. Advances in PE
research have been hampered owing to a nonstandardized definition of PE, until the definitionby the International Society of Sexual Medicine (ISSM) in 2009. Once the diagnosis of PE isestablished through a thorough history, a variety of medical therapies is available, includingtricyclic antidepressants, selective serotonin reuptake inhibitors (SSRIs), centrally acting opi-ates, phosphodiesterase 5 inhibitors and topical desensitizing creams. Most of these treat-ments increase the intravaginal ejaculation latency time (IELT) and patient satisfaction scores,with the most convincing evidence for SSRIs and topical creams. Daily SSRIs such as parox-etine, although efficacious, do have a substantial and prolonged side effect profile. Dapoxetine,which is a on-demand SSRI, is the only licensed drug for the treatment of PE, increasing IELTby a factor of 2.5 to 3 with limited and tolerable side effects. In the near future, the topicalaerosol PSD502 is due to be licensed for the treatment of PE, increasing IELT by up to a factorof 6 but having minimal local and negligible systemic side effects.
Keywords: male sexual dysfunction, medical therapy, medical treatment, prematureejaculation
arbitrary time of 1 minute from vaginal penetra-
Premature ejaculation (PE) can be a debilitating
tion to ejaculation was suggested by some
male sexual impairment. A range of studies have
[Marmor, 1976] while others defined the condi-
suggested a prevalence of 439% [Laumann et al.
tion in terms of the number of penile thrusts
1999; Grenier and Byers, 1995; Spector and
Carey, 1990; Nathan, 1986; Reading and West,
ejaculation [Colpi et al. 1986]. Other authors
1984]. This wide range can be partly attributed
added a more subjective element to the definition
to variations in the way that PE is defined, but
by defining PE as ejaculation that happens prior
may also reflect differences between populations
to when the male desires it [Hastings, 1963] or
ejaculations which are satisfactory to the female
Furthermore, because of the intimate nature of
partner in less than 50% of sexual intercourses
the problem, PE tends to be under-reported by
[Masters and Johnson, 1970]. A consensus on a
patients who do not typically seek medical help
Several attempts have been made over the years
Over the years, PE has been defined in various
by a number of major societies (WHO, APA,
ways. Some consider it controversial that PE is
EAU, AUA, ISSM) dealing with male sexual dys-
even considered to be a sexual dysfunction at all,
function to reach a consensus on the definition of
since all male upper mammalian species, includ-
PE. Table 1 illustrates the various definitions
ing primates ejaculate almost immediately on
penetration of the vagina [Wainberg, 1984].
All of the above definitions acknowledge one or
However, initial definitions of PE revolved
around ejaculation which regularly occurs at oraround initial vaginal penetration [Marmor,
1976]. A quantitative element was subsequently
added to the definition. For instance, the
Table 1. Early definitions of premature ejaculation.
The World Health Organisation (WHO) (International
An inability to delay ejaculation sufficiently to enjoy
Classification of Diseases-ICD, 1994) [WHO, 1994]
lovemaking, which manifests as either of the following:
occurrence of ejaculation before or very soon afterthe beginning of intercourse (within 15 seconds of thebeginning of intercourse)
occurrence of ejaculation in the absence of sufficienterection to make intercourse possible
Exclusion criteria: PE is not the result of prolonged
The American Psychiatric Association (APA) (The
Persistent or recurrent ejaculation with minimal
Diagnostic and Statistical Manual of Mental Disorders,
sexual stimulation before, on or shortly after pene-
Fourth Edition (DSM-IV), 2000) [APA, 2000]
tration and before the person wishes it. The distur-bance causes marked distress or interpersonaldifficulty.
Exclusion: PE is not due exclusively to the direct effects
of a substance (e.g. withdrawal from opioids) and fac-tors that affect duration of the excitement phase, suchas age, novelty of the sexual partner or situation, andrecent frequency of sexual activity.
The European Association of Urology (EAU) (Guidelines
The inability to control ejaculation for a sufficient
on Disorders of Ejaculation, 2001) [Colpi et al. 2001]
length of time before vaginal penetration.
Exclusion: Impairment of fertility does not happen when
The American Association of Urology (AUA) (Guidelines
Ejaculation that occurs sooner than desired, either
on the pharmacologic management of premature
before or shortly after penetration, causing distress to
ejaculation, 2004) [Montague et al. 2004]
In 2009, the International Society of Sexual
The impact of this new definition on the diagno-
Medicine (ISSM) [Althof et al. 2009] produced
sis and management of PE is awaited. In the
its guidelines of the diagnosis and management of
interim, the definition advocated by the authors
PE. It postulated an evidence-based definition of
PE and defined PE as a male sexual dysfunctioncharacterized by:
Diagnosis and classificationPE can be divided into two distinct entities:
. ejaculation which always or nearly always
acquired and lifelong PE [Godpodinoff, 1989].
occurs prior to or within about 1 minute of
Lifelong PE is a condition which has existed
since the onset of sexual activity and is not reliant
. inability to delay ejaculation on all or nearly
on either the conditions or the environment
under which sexual activity is taking place.
. negative personal consequences, such as dis-
Acquired PE develops in an individual who has
tress, bother, frustration and/or the avoidance
previously had normal ejaculatory control and
This definition is regarded as the most robust to
The cause of PE is usually not apparent. Some
date owing to its evidence-based nature and has
have characterized these cases as being psycho-
largely replaced the previous definitions as the
genic in origin, while others have postulated ‘bio-
2008]. This fundamental controversy about
However, the Diagnostic and Statistical Manual
of Mental Disorders, Fifth Edition (DSM-5) due
has been reflected in the two differing approaches
to be published in May 2013 [APA, 2013] may
to therapy (i.e. behavioural or psychotherapy ver-
offer an alternative take on the definition of PE.
sus pharmacological therapy). Those proposing a
psychogenic basis in the absence of a definitive
Classification of PE is still evolving as different
physical cause suggest that PE may be associated
classification models offer different clinical and
research benefits [Cahangirov et al. 2011; Chanet al. 2011; Cle´ment et al. 2009; Waldinger and
. novelty of partner or situation;. low frequency of sexual activity.
Biogenic PE is linked to an identifiable organic
Clinical history plays an important part in the
cause and the following conditions have been
diagnosis of PE since it is by definition a self-
reported diagnosis. However, clinical assessmentcan be challenging owing to the nature of the
problem. Patients may be embarrassed and shy
when relating details of their sexual experiences
and exact details are not forthcoming. It may
then be useful to involve the partner in the
Once the condition is treated, the expectation is
To elicit a diagnosis of PE, the three main com-
Those who have proposed biogenic theories for
ponents of PE (timing, control and satisfaction)
the development of PE have suggested that one of
should be specifically addressed. Once a diagno-
the following may be the pathophysiological
sis of PE is established, other related avenues that
. the nature of the PE (lifelong or acquired);
. the presence or absence of any associated
. the impact of the PE on the relationship with
. the impact of the PE on quality of life;. previous treatment (including over the coun-
Waldinger and Schweitzer introduced the con-
cept of PE as a syndrome, with patientsexperiencing
Examination of the patient involves a general
[Waldinger and Schweitzer, 2006]. The four
examination as well as a more focused examina-
tion of the genitalia outlining the scrotal contentsand the penis in detail. A digital rectal examina-
. short IELT, with control;. short IELT, no control;
tion to palpate the prostate gland is also recom-
mended. Questionnaires such as the Index of
Premature Ejaculation [Yuan et al. 2004] andthe
[Symonds et al. 2007] also have a role is evaluat-
include a category called ‘natural variable PE’
ing PE. It must be noted that the routine use of
whereby the episodes of PE are not consistent
questionnaires is not very useful, as they have a
and can be situational. This group falls under
tendency to confuse the picture, especially when
the umbrella ‘short IELT and no control’. This
ED occurs concurrently. ED specific question-
may represent a variation of natural ejaculatory
naires such as the IIEF and its shorter version,
function. Another category that stems from
IIEF-5, have been shown to further complicate
this syndrome is the ‘Premature-like ejacula-
the issue, especially in ED and PE trials
tory function’ whereby the patients perceive
IELTs fall in the normal range. This falls
Laboratory and other physiological tests are
rarely indicated. History and examination are
• Time to ejaculation• Perceived degree of ejaculatory control• Degree of bother• Onset and duration• Psychosocial and relationship issues• Medical history
• If PE secondary to ED, treat ED first
Attempt withdrawal of drug therapy after 6-8 weeks
Figure 1. Management of premature ejaculation. PE, premature ejaculation; ED, erectile dysfunction.
conclusive (after 3 years of follow up, 75% of
Treatment of PE can be a real challenge for the
men showed no lasting improvement) [Hawton
clinician (Figure 1). This is primarily because
et al. 1986]. One strategy, particularly for youn-
the pathophysiology of PE is so poorly under-
ger men suffering from PE, is precoitus mastur-
stood. Over the years multiple treatment modal-
bation which partially desensitizes the penis and
ities have been tried, often with initial promise.
leads to a delay in ejaculation [Sadeghi-Nejad
However, there are few studies on long-term effi-
cacy and durability for most of the currentlyavailable treatment options. This article aims to
Psychotherapy. Psychotherapy involves educat-
provide an overview of the different treatment
ing both the male patient and the female partner.
options available together with an assessment of
This can happen in the context of marriage/rela-
tionship counselling as well as psychosexual ther-apy [Hatzimouratidis et al. 2010]. Again short-
term results have been promising although
Psychological and behavioural therapy histori-
cally have a significant role in the managementof PE.
Behavioural therapy. The ‘stopstart’ strategy
The quest to develop an effective tablet to aid
(stopping coitus in situ and restarting after a
and ultimately cure PE has been ongoing for
delay) and its evolution to the ‘squeeze’ tech-
many decades [Schapiro, 1943]. A number of
nique (the physical application of pressure at
drugs have shown some promise in treating PE
the base of the head of the penis) have been
with varying degrees of success. At the present
time, only one drug (dapoxetine) is licensed (in
However, while short-term benefits have been
some countries only) for the treatment of PE.
reported (symptomatic benefit in 4565%), the
However, the other drugs described below can
long-term results of treatment have not been
also be used, as long as the patient is fully
aware that they are not licensed for the treatment
[Strassberg et al. 1999; Kim and Seo, 1998;
Segraves et al. 1993], with reports of improvedsexual satisfaction both from patients and part-
ners [Althof et al. 1995]. The use of clomipra-mine is limited by its associated side effects,
mainly fatigue, dizziness, dry mouth and hypo-
(Phenoxybenzamine, alfusozin, terazosin) and
tension. During continuous dosing, the adverse
monoamine oxidase inhibitor (Isocarboxazid,
event profile of clomipramine in men with PE
Phenelzine). Together with monoamine oxidase
was reported to be significantly worse than with
first oral medication used for the treatment ofPE.
SSRIs unlicensed (escitalopram, fluoxetine, flu-
voxamine, paroxetine, sertraline). Serotonergic
ited their use. These agents are not used for PE
agents have been shown to be effective in the
anymore [Beretta et al. 1986; Shilon et al.
1984; Aycock, 1949]. More selective alpha-
blockers such as terazosin have shown some
tor which leads to a delay of ejaculation [Lue and
promise in treating PE in patients suffering
Broderick, 2007; Waldinger et al. 1998]. The
from concurrent lower urinary tract symptoms
effect of SSRIs on the delay of ejaculation was
first noted by Patterson when treating men with
depression [Patterson, 1993]. Since then, studies
A range of drugs are currently used by clinicians
have shown that the effect of SSRIs to delay ejac-
for the management of PE including antidepres-
ulation can be seen within days of the start of
sants, local anaesthetic agents and phosphodies-
treatment with a plateauing of the effect within
4 weeks. In the variously reported studies theIELT is increased between twofold and eightfold
Whether the medication is used regularly or on
patients when choosing the most appropriate
The use of fluoxetine to treat PE was first
described in 1994 by Forster [Forster, 1994]
on-demand drug offers the flexibility of using
and Waldinger and colleagues conducted the
the medication just prior to sexual intercourse,
first randomized, controlled trial to evaluate the
thereby reducing the risks of side effects associ-
use of paroxetine in treating PE [Waldinger et al.
ated with the drug for the rest of the time. Data
1994]. Further work by the same research group
so far suggest that generally speaking the benefit
demonstrated efficacy of a number of SSRIs (flu-
of on-demand dosing is inferior to the benefits
oxetine, fluvoxamine, paroxetine and sertraline)
seen with regular dosing. On the other hand,
in the treatment of PE, although with varying
daily dosage allows for a more spontaneous
efficacy and side-effect profiles [Waldinger et al.
1998]. Fluoxetine, sertraline and paroxetine
dosing results in greater exposure to the drug
increased IELT significantly whereas there was
and may be associated with more pronounced
no statistical difference with fluvoxamine.
side effects. Waldinger and colleagues showedthat the majority of men (81%) preferred a
Kim and Seo demonstrated that treatment with
sertraline was nearly as effective and had a lower
regimen [Waldinger et al. 2007]. Moreover, the
incidence of side effects than clomipramine [Kim
stigma associated with the daily use of an antide-
and Seo, 1998]. Further studies (prospective
pressant (i.e. selective serotonin reuptake inhibi-
studies and randomized controlled trials) have
tors [SSRI]) may be a complicating factor in the
confirmed the efficacy of sertraline in the man-
compliance of patients to the treatment.
agement of PE [Balbay et al. 1998; Biri et al. 1998; Mendels, 1995]. Duloxetine [Athanasios
et al. 2007] and Escitalopram [Safarinejad,
2007] have also been shown to be effective in
on-demand dosing of clomipramine increases
treating PE. The efficacy and side-effects associ-
ated with SSRIs are described later (see Table 5).
Adverse effects with SSRIs are usually minor and
Dapoxetine is a drug specifically developed for
include fatigue, yawning, mild nausea, loose
the on-demand treatment of PE. It has been
stools and perspiration. They usually present at
extensively evaluated in five randomized, pla-
the beginning of the treatment and they tend to
cebo-controlled phase III clinical trials involving
disappear within 23 weeks. There have been
more than 6000 men with PE. This is the largest
and most comprehensive clinical trial programme
increased suicide risks with the use of SSRIs,
to date for a drug therapy to treat PE. It is a
short-acting SSRI designed to be taken only
et al. 2004; Kim and Seo, 1998; Waldinger
when needed and is taken 13 hours before
et al. 1998]. Therefore, it is important that
patients are adequately counselled about therisks involved with the use of these drugs.
There is evidence of its efficacy, its relatively
Once patients have been started on SSRI treat-
mundane side effect profile and its validity
ment, it is essential to perform follow-up assess-
as an on-demand medication [Feige et al. 2011;
ments to not only evaluate the efficacy of the drug
Hoy and Scott, 2010; Kaufman et al. 2009;
but also to identify any side effects, especially
McMahon et al. 2009; Giuliano et al. 2007].
regarding associated sexual dysfunction and sui-
However, the durability of the effects of dapoxe-
tine has not yet been demonstrated in prospec-tive, randomized trials since long-term follow upis not yet available [Safarinejad and Hosseini,
Licensed SSRI (dapoxetine). Dapoxetine is the
only licensed drug in the treatment of PE. Ithas been approved for treatment for the treat-
Table 2 summarizes the double-blind, random-
ment of PE in New Zealand, Sweden, Austria,
ized, placebo-controlled parallel trials to date
Finland, Germany, Spain, Italy and Portugal.
looking at the use of dapoxetine for the treatment
National approvals and licenses in five other
of PE [McMahon et al. 2011; Buvat et al. 2009;
European countries are expected to follow.
Kaufman et al. 2009; Patrick et al. 2009; Pryor
Dapoxetine is not approved for marketing in the
et al. 2006]. A total of 6081 patients were
Table 2. Treatment of premature ejaculation with dapoxetine (phase III clinical trials).
DizzinessSomnolenceHeadacheVomitingDiarrhoeaNasopharyngitis
Statistically significant improvement in:
Interpersonal difficulty related to ejaculation
IELT, intravaginal ejaculation latency time; PRN, pro re nata.
Desensitizing agents (SS Cream, benzocaine,
With this in mind there has been a move to
prilocaine, lidocaine). The use of a local anaes-
the use of aerosols which can be more discreet
thetic to desensitize the penis prior to coitus
and patient friendly [Dinsmore et al. 2007].
has been described since the middle part of
the last century [Damrau, 1963]. A number
caineprilocaine spray for use in PE, labelled
of these products are available as ‘over-the-coun-
PSD 502 has been tested in two early stage
ter’ medications and can be readily purchased
online. They predominantly come in the form
of creams although topical sprays are also
Wyllie, 2009; Dinsmore et al. 2007; Henry
and Morales, 2003]. The spray forms a clear,slightly oily, odourless solution that remains
Xin and colleagues published data demonstrating
that patients suffering from PE had an increased
condom required. It is easily wiped off, if nec-
vibratory threshold on the glans penis when it
essary, before penetration and the anaesthetic
penetrates the glans within 5 minutes although
(SS-Cream herbal cream). Moreover, the
it is not capable of penetrating intact kerati-
effect was dose related [Xin et al. 2000].
nised skin and will therefore not anaesthetize
Thereafter, the same research group performed
the shaft of the penis or the hands. Table 3
a randomized controlled trial demonstrating an
shows the efficacy and side effect profiles of
increase in IELT by eightfold when using the
Desensitizing creams and sprays can cause side
effects including hypoanaesthesia of the penile
(EMLA cream) and aerosol sprays have been
shaft and numbing of the vaginal vault of the
partner, unless a condom is used [Lue and
[Dinsmore et al. 2007; Henry and Morales,
Broderick, 2007]. Irritating local and systemiceffects have also been reported, although they
2003; Berkovitch et al. 1995] and in randomized,
are rare [Busato and Galindo, 2004; Atikeler
controlled trials [Carson and Wyllie, 2010;
Busato and Galindo, 2004]. The optimum timeof application of the EMLA cream has been
shown to be 20 minutes prior to intercourse
tadalafil). The role of PDE5 inhibitors (PDE5-
and the optimum concentration 5% [Atikeler
I) in the management of PE is controversial.
et al. 2002]. However, topical cream can be
Although a prospective study showed an increase
of IELT of a factor of 5.7 in patients using silden-
condom to minimize the effect of the cream
afil for the treatment of PE [Wang et al. 2007],
there still is minimal evidence to propose the use
Table 3. Treatment of PE with PSD 502 (randomized controlled trials).
Statistically significant improvement in:
Statistically significant improvement in:
IELT, intravaginal ejaculation latency time; PE, premature ejaculation; ED, erectile dysfunction.
Table 4. Randomized, controlled trials of PDE5-I.
Moderate increase in patient satisfaction
IELT, intravaginal ejaculation latency time; PE, premature ejaculation.
of PDE5-I in treating PE. Table 4 gives a sum-
on-demand medication, although the mechanism
mary of the randomized, controlled trials for
is poorly understood [Alghobary et al. 2010;
Salem et al. 2008; Safarinejad and Hosseini,2006]. However, there is evidence that some
Epidemiological studies have shown that a third
cases of secondary PE are seen in men who are
of men with ED suffer from PE [Corona et al.
withdrawing from opiate addiction. There may
2004]. This association between PE and ED
therefore be a relation between central opioid
may be explained by the fact that when a man
suffers from ED, he makes a compensatory effortto achieve ejaculation before the loss of the erec-
Table 5 gives a summary of the medication cur-
tion, leading to PE. A possible carry on effect
rently being used for the treatment of PE.
from this is when the man suffering from EDtries to overstimulate himself to achieve a rigid
erection, whereby this overstimulation leads to
Additional research is required to eventually
PE [Jannini et al. 2005]. Therefore, by treating
develop a product which is acceptable to the
the ED with PDE5 inhibitors, the corresponding
patient by being effective all of the time with min-
associated PE improves. However, evidence that
imal side effects and that is easy and discreet to
this mechanism is actually occurring is not forth-
use without compromising spontaneity during
coming as yet. There are just two randomized
sexual intercourse. Some of the possibilities are
controlled trials evaluating a PDE5-I in the man-
agement of PE [Aversa et al. 2009; McMahonet al. 2005].
. 9-hydroxycanthin-6-one (9-HC-6-one), a b-
carboline alkaloid isolated from Eurycoma
Although the evidences does not strongly support
longifolia. In vitro, it has been noted that 9-
the use of PDE5-I in primary PE, it may have a
HC-6-one attenuated PE-induced contrac-tion by blocking calcium channels [Chiou
role in treating PE in patients intolerant to
dapoxetine, especially if the PE is associated
. It has been noted that decreased levels of mag-
nesium may give rise to vasoconstrictionfrom
and decreased nitric oxide. This mechanism
(tramadol). Safarinejad and Hosseini have pub-
lished a randomized, controlled trial on the use of
tramadol HCL to treat PE [Safarinejad andHosseini, 2006]. Various research groups have
However, there is a long way to go before these
shown tramadol to have some efficacy in treating
products can be marketed. Moreover, reproduc-
PE [Alghobary et al. 2010], especially as an
ible in vitro and in vivo studies are required and
Table 5. Efficacy and side effects of drugs used in the management of PE.
IELT, intravaginal ejaculation latency time; PE, premature ejaculation; ED, erectile dysfunction; SSRI, selective serotonin reuptake inhibitor; PRN,pro re nata.
the formulation of a standardized definition of
PE is possibly the first building block towards
This research received no specific grant from any
funding agency in the public, commercial, or not-for-profit sectors. Conflict of interest statement
The authors declare no conflicts of interest in
PE is a common condition affecting around one
in five men. It can be a cause of significant per-sonal distress which may in turn affect the rela-
tionship of the man with his partner. While many
Alghobary, M.M.D., El-Bayoumy, Y.M.D., Mostafa,
men with PE do not seek medical attention, when
Y.M.D., Mahmoud, E.-H.M.M.D. and Amr, M.M.D.
they do, SSRIs, desensitizing creams and to a
(2010) Evaluation of tramadol on demand vs. daily
lesser extent PDE5-I have been used in the treat-
paroxetine as a long-term treatment of lifelong pre-mature ejaculation. J Sexual Med 7: 28602867.
ment. All of these medications are sold off-labelfor the treatment of PE except for the recently
Althof, S., Abdo, C., Dean, J., Hackett, G., McCabe,
licensed dapoxetine (PriligyTM) which provides
M., McMahon, C. et al. (2009) International Societyfor Sexual Medicine’s guidelines for the diagnosis and
an effective, on-demand treatment regimen with
treatment of premature ejaculation. http://www.issm.
relatively minimal side effects. PSD 502 is cur-
info/v4/. Accessed on 23 September 2011.
rently in the development phase and with the
Althof, S., Levine, S., Corty, E., Risen, C., Stern, E.
conclusion of phase III trials, may soon be
and Kurit, D. (1995) A double-blind crossover trial of
licensed as a topical aerosolised spray for the
clomipramine for rapid ejaculation in 15 couples.
APA. (2000) Diagnostic and Statistical Manual of
ejaculation: results of a phase III, double-blind, pla-
Mental Disorders. Washington, DC: American
cebo-controlled study. J Sex Med 7: 31793189.
Chan, J.S.W., Snoeren, E.M.S., Cuppen, E.,
APA (2013) Diagnostic and Statistical Manual of Mental
Waldinger, M.D., Olivier, B. and Oosting, R.S. (2011)
Disorders Development, 5th edition (DSM-5). Available
The serotonin transporter plays an important role in
at: http://www.dsm5.org/proposedrevision/pages/
male sexual behavior: a study in serotonin transporter
proposedrevision.aspx?rid¼174# (Accessed
knockout rats. J Sexual Med 8: 97108.
Athanasios, Z., Polyanthi, P. and George, K. (2007)
Hydroxycanthin-6-one induces penile erection and
The efficacy of duloxetine in the treatment of prema-
delays ejaculation. J Sexual Med DOI: 10.1111/
ture ejaculation. Int Urol Nephrol 39: 115118.
Atikeler, M., Gecit, I. and Senol, F. (2002) Optimum
Choi, H.K., Jung, G.W., Moon, K.H., Xin, Z.C.,
usage of prilocaine-lidocaine cream in premature
Choi, Y.D., Lee, W.H. et al. (2000) Clinical study of
ejaculation. Andologia 34: 356359.
SS-cream in patients with lifelong premature ejacula-tion1 1 SS-cream was developed originally by Drs. H.
Aversa, A., Pili, M., Francomano, D., Bruzziches, R.,
K. Choi and Z. C. Xin in Korea. The drug was sup-
Spera, E., La Pera, G. et al. (2009) Effects of vardenafil
ported and sponsored by the research fund of Cheil
administration on intravaginal ejaculatory latency time
Jedang Co. in Seoul, Korea. All authors have financial
in men with lifelong premature ejaculation. Int J Impot
interests and other relationships with SS-cream.
Aycock, L. (1949) The medical management of pre-
Cle´ment, P., Pozzato, C., Heidbreder, C., Alexandre,
L., Giuliano, F. and Melotto, S. (2009) Delay of
Balbay, M., Yildiz, M., S¸alvarci, A., O
Ejaculation Induced by SB-277011, a selective dopa-
¨ zbek, E. (1998) Treatment of premature ejaculation
mine D3 receptor antagonist, in the rat. J Sexual Med
with sertralin. Int Urol Nephrol 30: 8183.
Bas¸ar, M., Ylmaz, E., Ferhat, M., Bas¸ar, H. and
Colpi, G.M., Fanciullacci, F., Beretta, G., Negri, L.
Batislam, E. (2005) Terazosin in the treatment of
and Zanollo, A. (1986) Evoked sacral potentials in
premature ejaculation: a short-term follow-up. Int Urol
subjects with true premature ejaculation. Andrologia
Beretta, G., Chelo, E., Fanciullacci, F. and Zanollo, A.
Colpi, G. M., Hargreave, T.B., Papp, G. K., Pomerol,
(1986) Effect of an alpha-blocking agent (phenoxy-
J. M. and Weidner, W. (2001) Guidelines on disorders
benzamine) in the management of premature ejacula-
of ejaculation. European Association of Urology.
Available at: http://www.uroweb.org/fileadmin/user_upload/Guidelines/2001_Disorders_of_
Berkovitch, M., Keresteci, A. and Koren, G. (1995)
Efficacy of prilocaine-lidocaine cream in the treatmentof premature ejaculation. J Urol 154: 13601361.
Corona, G., Petrone, L., Mannucci, E., Jannini, E.A.,Mansani, R., Magini, A. et al. (2004) Psycho-biologi-
Biri, H., Isen, K., Sinik, Z., Onaran, M., Ku
cal correlates of rapid ejaculation in patients attending
and Bozkirli, I. (1998) Sertraline in the treatment of
an andrologic unit for sexual dysfunctions. Eur Urol
premature ejaculation: A double-blind placebo con-
trolled study. Int Urol Nephrol 30: 611615.
Damrau, F. (1963) Premature ejaculation: Use
Busato, W. and Galindo, C.C. (2004) Topical anaes-
of ethyl aminobenzoate to prolong coitus. J Urol
thetic use for treating premature ejaculation: a double-
blind, randomized, placebo-controlled study. BJU Int93: 10181021.
Dinsmore, W.W., Hackett, G., Goldmeier, D.,Waldinger, M., Dean, J., Wright, P. et al. (2007)
Buvat, J., Tesfaye, F., Rothman, M., Rivas, D.A. and
Giuliano, F. (2009) Dapoxetine for the treatment of
ejaculation (TEMPE): a novel aerosol-delivery
premature ejaculation: results from a randomized,
form of lidocaine-prilocaine for treating premature
double-blind, placebo-controlled phase 3 trial in 22
Dinsmore, W.W. and Wyllie, M.G. (2009) PSD502
Cahangirov, A., Cihan, A., Murat, N., Demir, O.,
improves ejaculatory latency, control and sexual satis-
Aslan, G., Gidener, S. et al. (2011) Investigation of the
faction when applied topically 5 min before intercourse
neural target level of hyperthyroidism in premature
in men with premature ejaculation: results of a phase
ejaculation in a rat model of pharmacologically
III, multicentre, double-blind, placebo-controlled
induced ejaculation. J Sexual Med 8: 9096.
Carson, C. and Wyllie, M. (2010) Improved ejacula-
Feige, A.M., Pinsky, M.R. and Hellstrom, W.J. (2011)
tory latency, control and sexual satisfaction when
Dapoxetine for Premature Ejaculation. Clin Pharmacol
PSD502 is applied topically in men with premature
Forster, P. (1994) Fluoxetine for premature ejacula-
Masters, W. and Johnson, V. (1970) Himan Sexual
Inadequacy. Boston, MA: Little, Brown & Co.
Giuliano, F., Bernabe, J., Gengo, P., Alexandre, L. and
McMahon, C., Althof, S., Kaufman, J., Buvat, J.,
Clement, P. (2007) Effect of acute dapoxetine
Aquilina, J., Rivas, D. et al. (2009) Efficacy and safety
administration on the pudendal motoneuron reflex in
of dapoxetine for premature ejaculation: integrated
anesthetized rats: comparison with paroxetine. J Urol
analysis of 5 phase 3 trials: PD-068. J Sexual Med
Godpodinoff, M. (1989) Premature ejaculation: clini-
McMahon, C., Kim, S.W., Park, N.C., Chang, C.-p.,
cal subgroups and etiology. J Sex Marital Ther
Rivas, D., Tesfaye, F. et al. (2011) Treatment of pre-
mature ejaculation in the Asia-Pacific region: resultsfrom a phase III double-blind, parallel-group study of
Grenier, G. and Byers, E. (1995) Rapid ejaculation: A
dapoxetine. J Sexual Med 7: 256268.
review of conceptual, etiological, and treatment issues. Arch Sex Behav 24: 447472.
McMahon, C.G., Abdo, C., Incrocci, L., Perelman,M., Rowland, D., Waldinger, M. et al. (2004)
Hastings, D. (1963) Impotence and Frigidity. Boston,
Disorders of orgasm and ejaculation in men. J Sexual
Hatzimouratidis, K., Amar, E., Eardley, I.,
McMahon, C.G., Stuckey, B.G.A., Andersen, M.,
Giuliano, F.H.D., Montorsi, F. et al. (2010)
Purvis, K., Koppiker, N., Haughie, S. et al. (2005)
Guidelines on male sexual dysfunction: Erectile
Efficacy of sildenafil citrate (Viagra) in men with pre-
dysfunction and premature ejaculation. Eur Urol,
mature ejaculation. J Sexual Med 2: 368375.
Mendels, J. (1995) Sertraline for premature ejacula-
Hawton, K., Catalan, J., Martin, P. and Fagg, J. (1986)
Long-term outcome of sex therapy. Behav Res Therapy24: 665675.
Mohammadreza, N., Mehdi, A. and Mohammad, H. (2009) Seminal plasma magnesium and premature
Henry, R. and Morales, A. (2003) Topical lidocaine-
ejaculation: a case-control study. Urol J 2: 102105.
prilocaine spray for the treatment of premature ejacu-lation: a proof of concept study. Int J Impot Res
Montague, D.K., Jarow, J., Broderick, G.A.,
Dmochowski, R.R., Heaton, J.P., Lue, T.F. et al. (2004) Premature Ejaculation: Guideline on the
Hoy, S.M. and Scott, L.J. (2010) Dapoxetine: in pre-
pharmacologic management of premature ejaculation.
mature ejaculation. Drugs 70: 14331443.
Jannini, E.A., Lombardo, F. and Lenzi, A. (2005)Correlation between ejaculatory and erectile dysfunc-
Nathan, S. (1986) The epidemiology of the DSM-III
psychosexual dysfunctions. J Sex Marital Ther12: 267281.
Kaufman, J.M., Rosen, R.C., Mudumbi, R.V.,Tesfaye, F., Hashmonay, R. and Rivas, D. (2009)
Patrick, D.L., Giuliano, F., Ho, K.F., Gagnon, D.D.,
Treatment benefit of dapoxetine for premature ejacu-
McNulty, P. and Rothman, M. (2009) The Premature
lation: results from a placebo-controlled phase III trial.
Ejaculation Profile: validation of self-reported outcome
measures for research and practice. BJU Int103: 358364.
Kim, S.C. and Seo, K.K. (1998) Efficacy andsafety of fluoxetine, sertraline and clomipra-
Patterson, W. (1993) Fluoxetine induced sexual dys-
mine in patients with premature ejaculation: a
function (letter). Clin Psychiatry 54: 71.
double-blind, placebo controlled study. J Urol
Pattij, T., Olivier, B. and Waldinger, M.D. (1995)
Animal models of ejaculatory behavior. Curr Pharm
Laumann, E., Paik, A. and Rosen, R. (1999) Sexual
dysfunction in the United States: Prevalence and pre-
Pryor, J.L., Althof, S.E., Steidle, C., Rosen, R.C.,
Hellstrom, W.J.G., Shabsigh, R. et al. (2006) Efficacy
Lue, T. and Broderick, G. (2007) Evaluation
and tolerability of dapoxetine in treatment of prema-
and nonsurgical management of erectile dysfunc-
ture ejaculation: an integrated analysis of two double-
tion and premature ejaculation, In: Walsh, P.,
blind, randomised controlled trials. Lancet
Retik, A., Vaughan, E., Wein, A., Kavoussi, L.,
Novick, A. et al. (eds). Campbell-Walsh Urology,
Ramanathan, R., Mulhall, J., Rao, S., Leung, R.,
Vol. 1, Philadelphia, PA: Saunders-Elsevier,
Martinez Salamanca, J.I., Mandhani, A. et al. (2007)
Predictive correlation between the International Index
Marmor, J. (1976) Impotence and ejaculatory distur-
of Erectile Function (IIEF) and Sexual Health
bances, In: Sadock, B., Kaplan, H. and Freedman, A.
Inventory for Men (SHIM): implications for calculat-
(eds). Sexual Experience. Baltimore, MD: The
ing a derived SHIM for clinical use. J Sexual Med
Williams & Wilkins Co, pp. 407410.
Reading, A. and West, W. (1984) An analysis of self-
Wainberg, J. (1984) Essai d’interpretation ontogene-
reported sexual behavior in a sample of normal males.
tique de l’ejaculation prematuree, In: Buvat, J. and
Jouaunnet, P. (eds). L’ejaculation et ses perturbances,Simep: Lyon-Villeurbanne, pp. 112116.
Sadeghi-Nejad, H. and Watson, R. (2008) Continuingmedical education: premature ejaculation: current
Waldinger, M., Hengeveld, M., Zwinderman, A. and
medical treatment and new directions (CME). J Sexual
Olivier, B. (1998) Effect of SSRI antidepressants on
ejaculation: a double-blind, randomized, placebo-controlled study with fluoxetine, fluvoxamine, parox-
Safarinejad, M.R.M.D. (2007) Safety and efficacy of
etine, and sertraline. J Clin Psychopharmacol
escitalopram in the treatment of premature ejaculation:
a double-blind, placebo-controlled, fixed-dose, ran-domized study. J Clin Psychopharmacol 27: 444450.
Wainberg, J. (1984) Essai d’interpretation ontogene-tique de l’ejaculation prematuree., In: Buvat, J. and
Safarinejad, M.R.M.D. and Hosseini, S.Y.M.D.
Jouaunnet, P., (eds), L’ejaculation et ses perturbances.
(2006) Safety and efficacy of tramadol in the treatment
Lyon-Villeurbanne: Simep, pp. 112116.
of premature ejaculation: a double-blind, placebo-controlled, fixed-dose, randomized study. J Clin
Waldinger, M.D. and Olivier, B. (2005) Animal
models of premature and retarded ejaculation. World JUrol 23: 115118.
Salem, E.A., Wilson, S.K., Bissada, N.K., Delk, J.R.,Hellstrom, W.J. and Cleves, M.A. (2008) ORIGINAL
Waldinger, M.D. and Schweitzer, D.H. (2006)
Changing paradigms from a historical DSM-III
Tramadol HCL has promise in on-demand use to treat
premature ejaculation. J Sexual Med 5: 188193.
definition of premature ejaculation. PartII—Proposals for DSM-V and ICD-11. J Sexual Med
Schapiro, B. (1943) Premature ejaculation: A review of
Waldinger, M.D., Zwinderman, A.H., Olivier, B. and
Segraves, R., Saran, A., Segraves, K. and Maguire, E.
Schweitzer, D.H. (2007) The majority of men
(1993) Clomipramine versus placebo in the treatment
with lifelong premature ejaculation prefer daily
of premature ejaculation: a pilot study. J Sex Marital
drug treatment: an observation study in a
consecutive group of Dutch men. J Sexual Med
Semans, J. (1956) Premature ejaculation: a new
Wang, W.-F., Wang, Y., Minhas, S. and Ralph, D.J.
Shilon, M., Paz, G. and Homonnai, Z. (1984) The use
(2007) Can sildenafil treat primary premature ejacu-
of phenoxybenzamine treatment in premature ejacu-
lation? A prospective clinical study. Int J Urol
Spector, I. and Carey, M. (1990) Incidence and
prevalence of the sexual dysfunctions: A critical review
International classification of diseases and related
of the empirical literature. Arch Sex Behav
health problems. Geneva: World Health Organization.
Xin, Z.C., Choi, Y.D., Lee, W.H., Choi, Y.J., Yang,
Strassberg, D., Brazao, C.d.G., Rowland, D., Tan, P.
W.J., Choi, H.K. et al. (2000) Penile vibratory thresh-
and Slob, A. (1999) Clomipramine in the treatment of
old changes with various doses of SS-cream in patients
rapid (premature) ejaculation. J Sex Marital Ther
with primary premature ejaculation. Yonsei Med J
Yuan, Y.M., Xin, Z.C., Jiang, H., Guo, Y.J., Liu, W.J.,
Symonds, T., Perelman, M.A., Althof, S., Giuliano, F.,
Martin, M., May, K. et al. (2007) Development and
Tian, L. et al. (2004) Sexual function of premature
validation of a premature ejaculation diagnostic tool.
ejaculation patients assayed with Chinese Index of
Premature Ejaculation. Asian J Androl 6: 121126.
More savings with the Join or renew as a Sam’s Plus™ Member and save even more with 10-30% savings on select name-brand and generic prescriptions.** Extra Value Quantity Extra Value Quantity Brand Diabetes Brand Devices and Supplies Generic Diabetes Brand OTC Brand Gastrointestinal Brand Heart Health Generic Heart Health Generic Gastrointestinal * Extra
PARTICIPATION REPORT OF THE DELEGATION OF INDIA TO THE 15TH SESSION OF THE FAO/WHO COORDINATING COMMITTEE FOR ASIA (21-24 NOVEMBER 2006, SEOUL, KOREA) The Indian delegation to the 15th Session of the FAO/WHO Coordinating Committee for Asia was led by Shri Rajesh Bhushan, Director, Ministry of Health &FW and consisted of Shri Prashant Goel, Deputy Secretary, Department of Commerce,
 Medical therapy for premature ejaculation
! The Author(s), 2011.
Medical therapy for premature ejaculation
! The Author(s), 2011.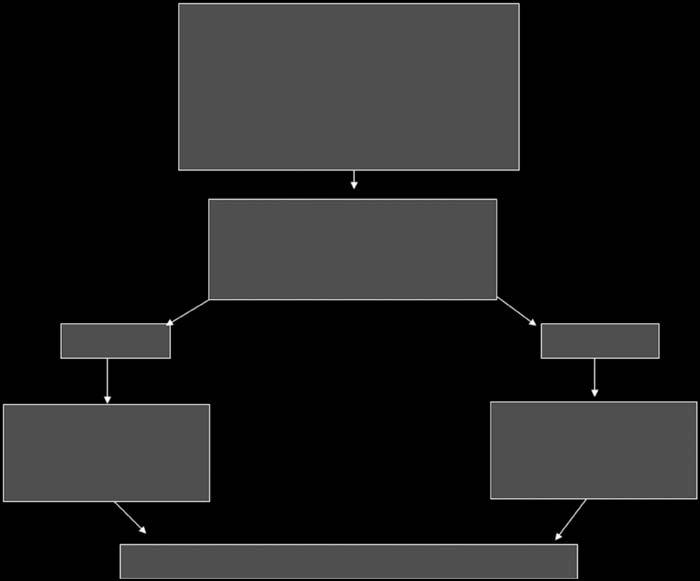 • Time to ejaculation• Perceived degree of ejaculatory control• Degree of bother• Onset and duration• Psychosocial and relationship issues• Medical history
• If PE secondary to ED, treat ED first
Attempt withdrawal of drug therapy after 6-8 weeks
Figure 1. Management of premature ejaculation. PE, premature ejaculation; ED, erectile dysfunction.
• Time to ejaculation• Perceived degree of ejaculatory control• Degree of bother• Onset and duration• Psychosocial and relationship issues• Medical history
• If PE secondary to ED, treat ED first
Attempt withdrawal of drug therapy after 6-8 weeks
Figure 1. Management of premature ejaculation. PE, premature ejaculation; ED, erectile dysfunction.