Association between physical activity, fiber intake, and other lifestyle variables and constipation in a study of women
Association Between Physical Activity, Fiber Intake,and Other Lifestyle Variables and Constipation in aStudy of WomenLaurent Dukas, M.D., Walter C. Willett, M.D., and Edward L. Giovannucci, M.D., Sc.D. Departments of Nutrition and Epidemiology, Harvard School of Public Health, Boston, Massachusetts;Channing Laboratory, Department of Medicine, Brigham and Women’s Hospital and Harvard MedicalSchool, Boston, Massachusetts; and Geriatric Department, University Hospital, Basel, SwitzerlandOBJECTIVE: Because the risk factors for constipation in the
2.5 million physician visits annually The greatest
general population are poorly defined, we examined the
number of physician visits for constipation occurs in
association between age, body mass index, and selected
adults 65 yr of age and older Patients tend to define
lifestyle and dietary factors with the prevalence of consti-
constipation in terms of function, such as straining, in-
pation in the Nurses’ Health Study.
complete defecation, and hard stool consistency Incontrast, physicians and investigators usually define con-
METHODS: A total of 62,036 women, aged 36 – 61 yr and
stipation by stool frequencies twice weekly or less. Ac-
free of cancer, responded to mailed questionnaires in 1980and 1982, which assessed bowel movement frequency, di-
cording to an international classification, individuals with
etary, and lifestyle factors. Constipation was defined as two
fewer than three bowel movements per week may be
considered to be constipated Depending on thedefinition of constipation, the reported prevalence is as
RESULTS: A total of 3327 women (5.4%) were classified as
high as 34% in older women (over age 65 yr) and
having constipation. Age and body mass index were in-
versely associated with constipation (p for trend Ͻ 0.0001).
Despite the high prevalence, morbidity, and substantial
In multivariate analysis, women who reported daily physical
cost as a result of physician visits and over-the-counter
activity had a lower prevalence of constipation (prevalence
laxatives, the etiology of constipation or low bowel move-
ratio [PR] ϭ 0.56, 95% CI ϭ 0.44 – 0.70). Women in the
ment frequency among adults in the general population has
highest quintile of dietary fiber intake (median intake 20
received little systematic investigation. Numerous possible
g/day) were less likely to experience constipation (PR ϭ
etiological factors have been proposed for idiopathic con-
0.64, 95% CI ϭ 0.57– 0.73) than women in the lowest
stipation, but their evaluation has frequently been from
quintile (median intake 7 g/day). The PR for constipation for
uncontrolled studies, short-term interventions, or anecdotal
women who both reported daily physical activity and were
reports. Data from large-scale epidemiological studies are
in the highest quintile of fiber intake was 0.32 (95% CI ϭ
sparse. Using data from the first National Health and Nu-
0.20 – 0.54) compared with those with physical activity less
trition Examination Survey, constipation was found to be
than once weekly and those who were in the lowest quintile
more frequent in women, those with daily inactivity, low
of fiber intake. Higher frequency of aspirin intake was
income, poor education, higher consumption of coffee and
associated with an increasing prevalence of constipation
tea, and with some dietary variables, including lower fruit
(PR ϭ 1.38, 95% CI ϭ 1.17–1.62). Current smoking and
alcohol use were inversely associated with constipation.
Because of the paucity of relevant data, we investi-
CONCLUSIONS: Our data suggest that moderate physical ac-
gated the associations between age, body mass index
tivity and increasing fiber intake are associated with sub-
(BMI), physical activity, dietary fiber intake, and other
stantial reduction in the prevalence of constipation in
selected lifestyle variables (suspected or known risk fac-
women. (Am J Gastroenterol 2003;98:1790 –1796. 2003
tors) with prevalence of constipation, defined as two or
fewer bowel movements weekly, in a large cohort ofwomen. Because of the detailed information on multipledemographic, dietary, and lifestyle data, and the large
INTRODUCTION
sample size, we were able to control for many factors
Constipation represents the most common outpatient diges-
simultaneously and to determine the independent influ-
tive complaint in the United States and accounts for about
Lifestyle Variables and Constipation in Women MATERIALS AND METHODS
the alternative analysis that included laxative users, laxativeuse was analyzed as a categorical variable (daily/weekly/
Study Population and Assessment of Variables
monthly/less than monthly laxative use).
The participants were a subset of women of the Nurses’
For age, BMI, postmenopausal status and hormone use,
Health Study, an ongoing prospective study among 121,700
smoking history, and aspirin use, we used the status of 1982,
female registered nurses in the United States. At enrollment
and for physical activity, alcohol, coffee, and fiber intake,
in 1976, participants, who were 30 –55 yr old and married,
we used the covariate status of 1980, the year the food-
completed a mailed questionnaire that inquired about known
frequency questionnaire was first administered. BMI
or suspected risk factors for cancer and cardiovascular dis-
physical activity fiber alcohol and coffee
ease, anthropometric measures, physical activity, reproduc-
have been shown previously to be reported with mod-
tive factors, other lifestyle exposures, family history of
erate-to-high accuracy using our methodology.
related diseases, and medical history. Beginning in 1980, a
Prevalence ratios (PRs) for constipation were estimated
semiquantitative food-frequency questionnaire was admin-
by the ORs and 95% CIs for each category of dietary and
istered. Physical activity was assessed through the following
other variables. In the multivariate analysis, the trends were
questions: “At least once a week, do you engage in any
tested using a single ordinal variable in a logistic regression
regular activity similar to brisk walking, jogging, bicycling,
model to represent the ordered categories of a prediction
etc, long enough to work up a sweat? If yes, how many
variable. The p values for the trends are two sided.
times per week?” Details of the design and follow-up of thiscohort have been described previously
Women provided information about their bowel move-
ment frequency on the 1982 Nurses’ Health Study question-
For all variables considered, results for the age-adjusted and
naire that was mailed to the entire cohort. Possible answers
for bowel movement frequency were more than once daily/daily/every other day/every 3– 4 days/every 5– 6 days/once
Age
a week, or less. On the 1982 questionnaire, we also queried
In the multivariate analysis, age was inversely associated
participants about use of laxatives, including softeners,
with constipation (p for trend Ͻ 0.0001). Compared with 35
bulking agents, and suppositories. Possible answers were
to 39-yr-old women, women aged 60 yr and older had a
laxative use daily/at least once a week/one to four times a
multivariate-adjusted PR of constipation of 0.41 (95% CI ϭ
month/less than once a month/never. The reasons for laxa-
tive use and type of laxatives were not assessed. BMI and Physical Activity
The analyses for this study were limited to women who
BMI was inversely related to constipation (p for trend Ͻ
responded to the bowel movement frequency question in
0.0001); women with a BMI Ͼ 29 kg/m2 had a multivariate-
1982 (n ϭ 92,106). We excluded women who reported a
adjusted PR of 0.48 (95% CI ϭ 0.39 – 0.58) compared with
diagnosis of ulcerative colitis before 1982 (n ϭ 651) or who
women with a BMI Ͻ 21 kg/m2. There was no association
reported a cancer diagnosis other than nonmelanoma skin
up to a BMI of 26 kg/m2; then, the risk decreased with
cancer preceding and including 1982 (n ϭ 3,015). Because
increasing BMI. Increased physical activity was associated
laxatives influence bowel movement frequency, we ex-
with a reduced prevalence of constipation (p for trend Ͻ
cluded laxative users from the main analysis (n ϭ 26,404),
0.0001). Women who reported physical activity two to three
but included them in an alternative analysis. A total of
times per week had a multivariate-adjusted PR of 0.65 (95%
62,036 women were included in the main analysis; of these,
CI ϭ 0.59 – 0.71) and women who reported daily physical
3,327 reported bowel movement frequency every third day
activity had a multivariate adjusted PR of 0.56 (95% CI ϭ
0.44 – 0.70) compared with women with physical activityless than once weekly. Statistical Analysis We used logistic regression models to control simulta- Medication, Including Aspirin Intake and
neously for multiple variables We included in the
Postmenopausal Hormone Use
models variables that are suspected or established risk fac-
Total number of medications was not associated with PR of
tors for constipation, defined as two or fewer bowel move-
constipation (p for trend ϭ 0.09). Women who used three or
ments weekly. Variables included age (six 5-yr categories),
more drugs per day (aspirin and hormone replacement not
BMI (10 categories), nonoccupational physical activity (fre-
included, but controlled for) had a PR of constipation of
quency of exposure; five categories), smoking history (nev-
1.00 (95% CI ϭ 0.75–1.34) compared with women who
er, past, current), aspirin use frequency (five categories),
took no drugs. Increasing frequency of aspirin intake was
number of medications (five categories), and intake of al-
associated with a higher prevalence of constipation (p for
cohol (six categories), coffee (six categories), and dietary
trend Ͻ 0.0001). Women who used 15 or more aspirin
fiber (quintiles). We also considered menopausal status and
tablets per week had a multivariate adjusted PR of 1.38
postmenopausal hormone replacement use as covariates. In
(95% CI ϭ 1.17–1.62) for constipation compared with
Dukas et al. Table 1. Association Between Physical Activity, Fiber Intake, and Other Lifestyle Factors and Prevalence of Constipation Among 60,036 Women
Ͻ21 21–21.9 22–22.9 23–23.9 24–24.9 25–25.9 26–26.9 27–27.9 28–28.9
Ref. 0.95–1.28 0.92–1.23 0.87–1.17 0.86–1.17 0.88–1.20 0.73–0.99 0.69–0.98 0.50–0.73 0.39–0.58
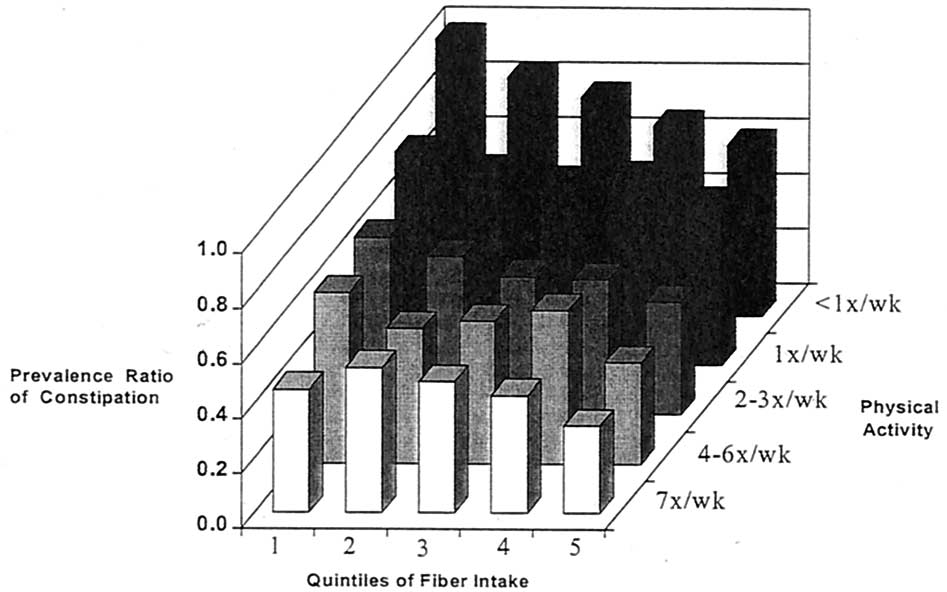
* Multivariate PR is from a logistic regression model containing age, BMI, smoking status, postmenopausal hormone use and status, physical activity, aspirin use, number ofmedications, alcohol, coffee, and fiber intake. Lifestyle Variables and Constipation in Women Figure 1. Combination of physical activity and fiber intake and prevalence of constipation.
women who never used aspirin. Postmenopausal hormone
daily fiber intake was relatively low for the whole cohort (12
use was not associated with constipation (multivariate-ad-
g daily), and only 1% had a fiber intake of more than 30 g
justed PR ϭ 1.07, 95% CI ϭ 0.95–1.23) for women with
current hormone use compared with women who never used
In a further analysis we classified women simul-
taneously by both physical activity and dietary fiber intake. In the multivariate analysis, the PR for constipation for
Smoking, Alcohol, and Coffee Consumption
women who both reported daily physical activity and were
Relative to never smoking, current smoking was associated
in the highest quintile of fiber intake was 0.32 (95% CI ϭ
with a slightly reduced multivariate-adjusted risk (PR ϭ
0.20 – 0.54) compared with those with physical activity less
0.81, 95% CI ϭ 0.74 – 0.89), whereas past smoking had no
than once weekly and those who were in the lowest quintile
association with constipation (PR ϭ 1.04, 95% CI ϭ 0.95–
of fiber intake. For women who reported physical activity
1.13). Daily alcohol consumption was inversely associated
two to three times per week and were in the highest quintile
with constipation (p for trend Ͻ 0.0001), though at least one
of fiber intake, the PR of constipation was 0.41 (95% CI ϭ
drink (approximately 12 g of alcohol) per day was required
0.33– 0.50) compared with those with physical activity less
to observe the lower prevalence. Women with a median
than once weekly and those who were in the lowest quintile
daily alcohol intake of 30.4 g had a multivariate adjusted PR
of fiber intake. The alternative analysis including laxative
of 0.66 (95% CI ϭ 0.57– 0.77) compared with women who
users showed similar results as the main analysis (data not
did not drink alcohol. Coffee intake seemed to have a
nonlinear relation with constipation. Women who drank sixor more cups of coffee daily had a slightly increased mul-tivariate-adjusted PR of 1.17 (95% CI ϭ 1.02–1.34) for
DISCUSSION
constipation compared with women who did not drink cof-fee. Low coffee intake (one cup/day or less), however, was
Constipation is common in Western countries possibly
inversely associated with constipation (PR for one cup/day
related to diet and lifestyle factors. Our study found that
ϭ 0.79, 95% CI ϭ 0.69–0.91) compared with women who
regular physical exercise and higher fiber intake were asso-
ciated with reduced risk of constipation even after control-ling for numerous factors. Women who were physically
Dietary Fiber
active daily and had approximately 20 g daily of fiber had a
Higher dietary fiber intake was associated with a decreased
3-fold lower prevalence of constipation compared with
prevalence of constipation (p for trend Ͻ 0.0001), even
women who rarely exercised and had about 7 g daily of
though the median fiber intake for women in the highest
quintile was 20 g daily, which is below the recommended
Some authors suggest that low bowel movement
fiber intake of 30 g/day. Women in the highest quintile of
frequency is associated with functional abnormalities of the
fiber intake had a multivariate adjusted PR of 0.64 (95% CI
colon, which usually tend to worsen with aging. However,
ϭ 0.57–0.73) compared with women in the lowest quintile
in our study, as well as in other studies age was
of fiber intake (median daily fiber intake of 7 g). The median
inversely associated with bowel movement frequency. Co-
Dukas et al.
lonic transit may slow with aging but is highly variable
was associated with a 2-fold risk of constipation Ex-
Although the majority of older people have stool frequen-
ercise increases propulsive movements in the large intestine
cies in the normal range, laxative use increases with aging
and hormonal changes and mechanical effects during
The study of Whitehead et al. showed that the use
exercise may alter GI function. Other mechanisms for the
of laxatives is affected more by the desire to have a bowel
influence of exercise are possible. For example, higher en-
movement than by actual frequency Furthermore, the
ergy expenditure increases energy intake requirements,
increase in laxative use with aging may result from
which may influence the total amount of dietary fiber con-
the elderly having more defecation problems such as strain-
sumed. However, in our analyses, controlling for fiber and
ing or suffering from hard stool consistency
further for energy intake did not appreciably change the
Another possible explanation for the inverse association
results for physical activity. As shown in the
between age and low bowel movement frequency in women
associations for physical activity and fiber and bowel move-
may be the decreasing estrogen plasma levels after meno-
ment frequency were independent. The lowest risk was in
pause. Increasing estrogen in the luteal phase of the men-
the most active women with the highest fiber intake. Thus,
strual cycle is associated with prolonged intestinal transit
the combination of a high-fiber diet and a high level of
time and diseases related to increased estrogen plasma
physical activity would tend to lead to the lowest risk for
levels have been shown to be associated with low bowel
movement frequency (27–29). Data are not available about
The linearly increasing risk of constipation with increas-
bowel movement frequency and aging in men in our study.
ing aspirin intake was also seen in two cross-sectional
However, most studies show that men are less likely to
studies and in several large case– control studies
suffer from constipation than women (4, 6, 7, 30). In our
and trials Constipation as a side effect is also
study, current postmenopausal hormone use was associated
known for other nonsteroidal anti-inflammatory drugs
with a slight, though not statistically significant, increased
The mechanism by which nonsteroidal anti-inflamma-
risk of low bowel movement frequency.
tory drugs reduce bowel movement frequency remains un-
Increasing BMI was inversely associated with low bowel
movement frequency. In other studies BMI had
Our finding that smoking is inversely associated with
no influence on colonic transit times or bowel movement
constipation is supported by two other studies In a
frequency. The reason for this inverse association is not
study by Cummings et al. smoking withdrawal in-
clear. However, within the normal range of BMI (Ͻ26
duced constipation, and in a study by Rausch et al.
kg/m2), we observed no relation with constipation.
transdermal application of nicotine increased rectosigmoidal
We found an inverse association between physical activ-
emptying, suggesting that nicotinic acid may influence
ity and low bowel movement frequency. In our study, phys-
ical activity only two to six times a week was associated
Alcohol intake exceeding 12 g/day was inversely associ-
with a 35% lower risk of constipation and daily activity with
ated with constipation. Alcohol withdrawal has been asso-
a 44% lower risk relative to less than once daily. A review
ciated with increasing intestinal transit time and heavy
of studies of the influence of exercise on the GI tract
alcohol consumption is associated with diarrhea be-
indicates that the urge to defecate and bowel movements are
cause of inflammation of the colonic mucosa and neurotox-
frequently reported during and after exercise However,
icity observed with alcohol However, we observed
results from other studies on the association between low
an inverse association at moderate levels that are unlikely to
bowel movement frequency and physical activity are incon-
be associated with these adverse effects of heavy drinking.
sistent. One crossover trial found a significant decrease
Coffee intake of more than six cups per day was associ-
in whole gut transit time during the exercise period, but
ated with a slightly increased risk of low bowel movement
defecation frequency did not change. Another trial in
frequency, whereas low-to-moderate consumption was as-
healthy young men and one trial in young healthy
sociated with a reduced risk of constipation. In the study by
subjects found no association between moderate physical
Sandler et al. constipated subjects reported higher con-
activity and bowel transit All three trials included
sumption of coffee compared with controls. Coffee is
small numbers of subjects, and none included reports of the
known to induce an increase in colonic motility limited to
subjects’ bowel habits. In another study two groups,
the rectosigmoid region within 4 min of ingestion and last-
one of which trained for 30 min at 70 – 80% of age-predicted
ing at least 3 min This influence of coffee on rectosig-
maximal heart rate three times weekly for 6 wk, were tested
moid responses appeared primarily in men and women who
before and after the training program. Although the running
claimed that coffee induced a desire to defecate (53% of
group’s average transit time decreased from 35 to 24 h, the
women and 19% of men). The speed of the response indi-
control group remained unchanged at 45 h Contrary to
cated that coffee may induce a gastrocolonic response, pos-
most trials, several other cross-sectional studies found an
sibly by acting on receptors in the stomach or small bowel
inverse association between physical activity and constipa-
and mediated by neural mechanisms or by GI hormones.
Our observed association between large amounts of coffee
Nutrition Examination Survey, low physical activity level
and low constipation might be a result of coffee-induced
Lifestyle Variables and Constipation in Women
diuresis leading to dehydration, which has been associated
ACKNOWLEDGMENTS
with constipation or to other unknown mechanisms.
Associations between dietary factors and constipation
The work reported in this manuscript was supported by
should be interpreted with caution because the reported diet
CA40356, the main Nurses’ Health Study grant. The study
may reflect changes in food decision caused by constipation.
was last reviewed and approved by the Human Research
In our study, fiber intake was inversely associated with low
Committee on July 18, 2002 (Protocol # 1999-P-011114/7).
bowel movement frequency. In intervention trials, addingfiber to specific diets increased bowel movement frequency
Reprint requests and correspondence: Edward Giovannucci,
The positive relationship between fiber intake and
M.D., Sc.D., Harvard School of Public Health, 665 Huntington
stool weight is well established Other studies found a
weak or null association between fiber intake and bowel
Received Nov. 21, 2002; accepted Feb. 24, 2003.
movement frequency possibly because ofsmall sample size or a tendency for people who sufferedfrom constipation to increase their fiber intake. In our study,
REFERENCES
the combination of higher fiber intake and regular physical
1. Sonnenberg A, Koch TR. Physician visits in the United States
activity was associated with a large decrease in prevalence
for constipation: 1958 to 1986. Dig Dis Sci 1989;34:606 –11.
of constipation. We are not aware of any study that exam-
2. Sandler RS, Drossman DA. Bowel habits in young adults not
ined the combination of these variables.
seeking health care. Dig Dis Sci 1987;32:841–5.
The large size of our study (62,036 women) allowed us to
3. Preston DM, Lennard-Jones JE. Severe chronic constipation of
young women: ‘idiopathic slow transit constipation.’ Gut
examine several demographic and dietary characteristics for
a more complete description of low bowel movement fre-
4. Connell AM, Hilton C, Irvine G, et al. Variation of bowel habit
quency in U.S. women. A major strength of our study is the
in two population samples. Br Med J 1965;5470:1095–9.
ability to control for known or suspected risk factors for low
5. Stewart RB, Moore MT, Marks RG, et al. Correlates of con-
bowel movement frequency. One limitation of our study is
stipation in an ambulatory elderly population. Am J Gastro-enterol 1992;87:859 –64.
that the question about bowel movement frequency was
6. Hale WE, Perkins LL, May FE, et al. Symptom prevalence in
based strictly on self-report. However, nurses in this popu-
the elderly. An evaluation of age, sex, disease, and medication
lation have been shown to report a variety of medical factors
use. J Am Geriatr Soc 1986;34:333–40.
with high accuracy. Although there are alternative ways to
7. Whitehead WE, Drinkwater D, Cheskin LJ, et al. Constipation
assess constipation, bowel movement frequency can be used
in the elderly living at home. Definition, prevalence, and
most feasibly in a large population. However, bowel move-
relationship to lifestyle and health status. J Am Geriatr Soc1989;37:423–9.
ment frequency represents only one component of the spec-
8. Sandler RS, Jordan MC, Shelton BJ. Demographic and dietary
trum of constipation, and whether the same relationships we
determinants of constipation in the US population. Am J
observed would hold for other clinical subtypes of consti-
9. Giovannucci E, Colditz GA, Stampfer MJ, et al. A prospective
Another limitation is that we may have underestimated
study of cigarette smoking and risk of colorectal adenoma and
absolute fiber intake because our food-frequency question-
colorectal cancer in U.S. women. J Nat Cancer Inst 1994;86:192–9.
naire in 1980 did not assess all sources of fiber. However,
10. Platz EA, Martinez ME, Grodstein F, et al. Parity and other
this diet questionnaire adequately ranked individuals by
reproductive factors and risk of adenomatous polyps of the
quintile of fiber intake, and in a subset of participants who
distal colorectum (United States). Cancer Causes Control
completed detailed daily dietary records, the absolute in-
takes of fiber assessed by questionnaire and by dietary
11. Cupples LA, D’Agostino RB, Anderson K, et al. Comparison
of baseline and repeated measure covariate techniques in the
records were comparable We do not know if higher
Framingham Heart Study. Stat Med 1988;7:205–22.
intakes of fiber would further reduce risk of constipation.
12. Rimm EB, Stampfer MJ, Colditz GA, et al. Validity of self-
Another limitation is also that we did not assess fluid intake
reported waist and hip circumferences in men and women.
in the 1980 food-frequency questionnaire, so we could not
exclude residual confounding by water intake.
13. Chasan-Taber S, Rimm EB, Stampfer MJ, et al. Reproducibil-
A variety of lifestyle factors may influence the risk of
ity and validity of a self-administered physical activity ques-tionnaire for male health professionals. Epidemiology 1996;
constipation. Some of these factors, particularly regular
physical activity and higher fiber intake, seem to be bene-
14. Hu FB, Rimm E, Smith-Warner SA, et al. Reproducibility and
ficial regarding constipation. Combining regular physical
validity of dietary patterns assessed with a food-frequency
activity and increasing fiber intake may represent an impor-
questionnaire. Am J Clin Nutr 1999;69:243–9.
tant, inexpensive, and feasible therapeutic measure for this
15. Giovannucci E, Colditz G, Stampfer MJ, et al. The assessment
of alcohol consumption by a simple self-administered ques-
widespread digestive complaint. The possible influence of
tionnaire. Am J Epidemiol 1991;133:810 –7.
other factors, including BMI, aspirin use, alcohol, and cof-
16. Grobbee DE, Rimm EB, Giovannucci E, et al. Coffee, caffeine
fee, on bowel movement frequency need to be considered in
and cardiovascular disease in men. N Engl J Med 1990;323:
relation to their other effects on overall health status. Dukas et al.
17. Burkitt DP. Epidemiology of cancer of the colon and rectum.
running program on bowel transit time. J Sports Med Phys
18. Waller SL, Misiewicz JJ. Colonic motility in constipation and
37. Campbell AJ, Busby WJ, Horwath CC. Factors associated
diarrhea. Scand J Gastroenterol 1972;7:93–6.
with constipation in a community based sample of people aged
19. Meunier P, Rochas A, Lambert R. Motor activity of the
70 years and over. J Epidemiol Comm Health 1993;47:23–6.
sigmoid colon in chronic constipation: Comparative study
38. Holdstock DJ, Misiewicz JJ, Smith T, et al. Propulsion (mass
with normal subjects. Gut 1979;20:1095–101.
movements) in the human colon and its relationship to meals
20. Frieri G, Parisi F, Corazziari E, et al. Colonic electromyogra-
and somatic activity. Gut 1970;11:91–9.
phy in chronic constipation. Gastroenterology 1983;84:737–
39. Talley NJ, Weaver AL, Zinsmeister AR, et al. Functional
constipation and outlet delay: A population-based study. Gas-
21. Bueno L, Fioramonti J, Ruckebusch Y, et al. Evaluation of
colonic myoelectrical activity in health and functional disor-
40. Meade TW, Roderick PJ, Brennan PJ, et al. Extra-cranial
bleeding and other symptoms due to low dose aspirin and low
22. Milne JS, Williamson J. Bowel habit in older people. Gerontol
intensity oral anticoagulation. Throm Haemostas 1992;68:1–6.
41. Harker LA, Boissel JP, Pilgrim AJ, et al. Comparative safety
23. Dent OF, Goulston KJ, Zubrzycki J, et al. Bowel symptoms in
and tolerability of clopidogrel and aspirin: Results from CA-
an apparently well population. Dis Colon Rectum 1986;29:
PRIE. CAPRIE Steering Committee and Investigators. Clopi-
dogrel versus aspirin in patients at risk of ischaemic events.
24. Everhart JE, Go VL, Johannes RS, et al. A longitudinal survey
of self-reported bowel habits in the United States. Dig Dis Sci
42. Wright MG. Micro-encapsulated aspirin (Levius) compared
with aloxiprin (Palaprin Forte) in the treatment of rheumatoid
arthritis. J Int Med Res 1976;4:272–5.
25. Madsen JL. Effects of gender, age, and body mass index on
43. Peto R, Gray R, Collins R, et al. Randomised trial of prophy-
gastrointestinal transit times. Dig Dis Sci 1992;37:1548 –53.
lactic daily aspirin in British male doctors. BMJ 1988;296:
26. Wald A, Van Thiel DH, Hoechstetter L, et al. Gastrointestinal
transit: The effect of the menstrual cycle. Gastroenterology
44. Cummings KM, Giovino G, Jaen CR, et al. Reports of smok-
ing withdrawal symptoms over a 21 day period of abstinence.
27. Corraziari E, Bausano G, Torsoli A, et al. Italian cooperative
study on chronic constipation. Ital J Gastroenterol 1981;13:
45. Rausch T, Beglinger C, Alam N, et al. Effect of transdermal
application of nicotine on colonic transit in healthy nonsmok-
28. Preston DM, Rees LH, Lennard-Jones JE. Gynaecological
ing volunteers. Neurogastroenterol Motil 1998;10:263–70.
disorders and hyperprolactinaemia in chronic constipation.
46. Bouchoucha M, Nalpas B, Berger M, et al. Recovery from
disturbed colonic transit time after alcohol withdrawal. Dis
29. Watier A, Devroede G, Duranceau A, et al. Constipation with
colonic inertia. A manifestation of systemic disease? Dig Dis
47. Papa A, Tursi A, Cammarota G, et al. Effect of moderate and
heavy alcohol consumption on intestinal transit time. Panmin-
30. Jones RH, Tait CL. Gastrointestinal side-effects of NSAIDs in
the community. Br J Clin Pract 1995;49:67–70.
48. Brown SR, Cann PA, Read NW. Effect of coffee on distal
31. Towers AL, Burgio KL, Locher JL, et al. Constipation in the
colon function. Gut 1990;31:450 –3.
elderly: Influence of dietary, psychological, and physiological
49. Davies L, Holdsworth MD, MacFarlane D. Dietary fibre in-
factors. J Am Geriatr Soc 1994;42:701–6.
takes in the United Kingdom before and after retirement from
32. Moses FM. The effect of exercise on the gastrointestinal tract.
work. Hum Nutr Appl Nutr 1986;40:431–9.
50. Astrup A, Vrist E, Quaade F. Dietary fibre added to very low
33. Oettle GJ. Effect of moderate exercise on bowel habit. Gut
calorie diet reduces hunger and alleviates constipation. Int J
34. Coenen C, Wegener M, Wedmann B, et al. Does physical
51. Rigaud D, Ryttig KR, Leeds AR, et al. Effects of a moderate
exercise influence bowel transit time in healthy young men?
dietary fibre supplement on hunger rating, energy input and
faecal energy output in young, healthy volunteers. A random-
35. Bingham SA, Cummings JH. Effect of exercise and physical
ized, double-blind, cross-over trial. Int J Obes 1987;11:73–8.
fitness on large intestinal function. Gastroenterology 1989;97:
52. Chen HL, Haack VS, Janecky CW, et al. Mechanisms by
which wheat bran and oat bran increase stool weight in hu-
36. Cordain L, Latin RW, Behnke JJ. The effects of an aerobic
mans. Am J Clin Nutr 1998;68:711–9.
Vi è indubbiamente un legame molto stretto tra i canti popolari e la città di Chioggia, un rapporto connesso alle caratteristiche strutturali, urbanistiche, sociali ed antropologiche della città, che va alle sue radici. Uno degli aspetti caratterizzanti del centro lagunare è costituito infatti dalla sua popolosità, un dato da intendere sia in senso quantitativo, relativo al considerevole i
LA RECHERCHE DOCUMENTAIRE BIOMEDICALE Via le Système d’Information Documentaire (SID) de la BIU de INTRODUCTION : L’ENVIRONNEMENT DOCUMENTAIRE UNIVERSITAIRE La Bibliothèque Interuniversitaire de Montpellier (BIU) est un réseau de 12 bibliothèques universitaires au service des 3 universités de Le Système d’Information Documentaire Les BU de médeci
 Lifestyle Variables and Constipation in Women
Lifestyle Variables and Constipation in Women