La spécificité du tadalafil est liée à sa longue demi-vie, permettant une action qui excède largement celle des autres inhibiteurs de PDE5. L’absorption digestive est complète, avec un pic plasmatique atteint en 2 heures environ. Le métabolisme est réalisé via CYP3A4, produisant des métabolites inactifs éliminés principalement dans les fèces. La sélectivité enzymatique est élevée, réduisant les effets indésirables extra-caverneux. Les réactions indésirables fréquentes incluent céphalées, bouffées vasomotrices et troubles digestifs légers. L’activité pharmacologique est stable, indépendamment de l’ingestion d’aliments. Dans les comparaisons de longue durée, acheter cialis pas cher est mentionné en relation avec les études portant sur la persistance d’efficacité et la constance de la cinétique plasmatique.
Cybernephrology.ualberta.ca
FIGURE 3-24
Approach to hyperkalemia: hyperkalemiawith reduced glomerular filtration rate(GFR). Normokalemia can be maintained in patients who consume normal quantitiesof potassium until GFR decreases to lessthan 10 mL/min; however, diminished GFRpredisposes patients to hyperkalemia fromexcessive exogenous or endogenous potassi-um loads. Hidden sources of endogenous andexogenous potassium—and drugs that pre-dispose to hyperkalemia—are listed.
FIGURE 3-25
Approach to hyperkalemia: hyporeninemichypoaldosteronism. Hyporeninemic hypoal-dosteronism accounts for the majority ofcases of unexplained hyperkalemia in patientswith reduced glomerular filtration rate (GFR)whose level of renal insufficiency is not whatwould be expected to cause hyperkalemia. Interstitial renal disease is a feature of mostof the diseases listed. The transtubular potassium gradient (see Fig. 3-26) can beused to distinguish between primary tubuledefects and hyporeninemic hypoaldostero-nism. Although the transtubular potassiumgradient should be low in both disorders,exogenous mineralocorticoid would normal-ize transtubular potassium gradient inhyporeninemic hypoaldosteronism.
Disorders of Water, Electrolytes, and Acid-Base
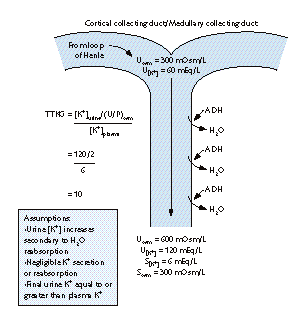
FIGURE 3-26
Physiologic basis of the transtubular potassium concentration gradient (TTKG). Secretion of potassium in the cortical collectingduct and outer medullary collecting duct accounts for the vastmajority of potassium excreted in the urine. Potassium secretion inthese segments is influenced mainly by aldosterone, plasma potassi-um concentrations, and the anion composition of the fluid in thelumen. Use of the TTKG assumes that negligible amounts of potassi-um are secreted or reabsorbed distal to these sites. The final urinarypotassium concentration then depends on water reabsorption in themedullary collecting ducts, which results in a rise in the final urinarypotassium concentration without addition of significant amounts ofpotassium to the urine. The TTKG is calculated as follows:
The ratio of (U/P)osm allows for “correction” of the final urinarypotassium concentration for the amount of water reabsorbed in the medullary collecting duct. In effect, the TTKG is an index of thegradient of potassium achieved at potassium secretory sites, indepen-dent of urine flow rate. The urine must at least be iso-osmolal withrespect to serum if the TTKG is to be meaningful [20]. FIGURE 3-27 CAUSES FOR HYPERKALEMIA WITH AN
Clinical application of the transtubular potassium gradient (TTKG). INAPPROPRIATELY LOW TTKG THAT IS UNRESPONSIVE
The TTKG in normal persons varies much but is genarally within
TO MINERALOCORTICOID CHALLENGE
the the range of 6 to 12. Hypokalemia from extrarenal causes resultsin renal potassium conservation and a TTKG less than 2. A highervalue suggests renal potassium losses, as through hyperaldostero-nism. The expected TTKG during hyperkalemia is greater than 10.
An inappropriately low TTKG in a hyperkalemic patient suggests
hypoaldosteronism or a renal tubule defect. Administration of the
mineralocorticoid 9 ␣-fludrocortisone (0.05 mg) should cause TTKG
to rise above 7 in cases of hypoaldosteronism. Circumstances are
listed in which the TTKG would not increase after mineralocorticoid
challenge, because of tubular resistance to aldosterone [21].
Sickle cell diseaseUrinary tract obstructionPseudohypoaldosteronism type I
FIGURE 3-28
Approach to hyperkalemia: low aldosteronewith normal to increased plasma renin. Heparin impairs aldosterone synthesis byinhibiting the enzyme 18-hydroxylase. Despite its frequent use, heparin is rarelyassociated with overt hyperkalemia; thissuggests that other mechanisms (eg, reducedrenal potassium secretion) must be presentsimultaneously for hyperkalemia to mani-fest itself. Both angiotensin-convertingenzyme inhibitors and the angiotensin type1 receptor blockers (AT1) receptor blockersinterfere with adrenal aldosterone synthesis. Generalized impairment of adrenal corticalfunction manifested by combined glucocor-ticoid and mineralocorticoid deficiencies areseen in Addison’s disease and in defects ofaldosterone biosynthesis.
FIGURE 3-29
Approach to hyperkalemia: pseudohypoaldosteronism. The mecha-nism of decreased potassium excretion is caused either by failure to secrete potassium in the cortical collecting tubule or enhancedreabsorption of potassium in the medullary or papillary collectingtubules. Decreased secretion of potassium in the cortical andmedullary collecting duct results from decreases in either apicalsodium or potassium channel function or diminished basolateralNa+-K+-ATPase activity. Alternatively, potassium may be secretednormally but hyperkalemia can develop because potassium reab-sorption is enhanced in the intercalated cells of the medullary col-lecting duct (see Fig. 3-4). The transtubule potassium gradient(TTKG) in both situations is inappropriately low and fails to nor-malize in response to mineralocorticoid replacement.
Advance Access Publication 7 February 2007Juice Powder Concentrate and Systemic Blood Pressure,Progression of Coronary Artery Calcium and AntioxidantStatus in Hypertensive Subjects: A Pilot StudyM. C. Houston1, B. Cooil2, B. J. Olafsson3 and P. Raggi41Hypertension Institute of Nashville, Vanderbilt University School of Medicine and Saint Thomas Hospital,2Owen Graduate School of Management, Vand
2005 Accomplishments General Accomplishments • Put on CASQA’s inaugural conference in October in Ontario, at which over 400 people and • CASQA membership increased to over 160 memberships during its’ third year • Continued to issue the bi-weekly CASQA Update to provide CASQA and stormwater news to members, issued 26 updates and 3 Alerts in 2005 CASQA Update , meeting not

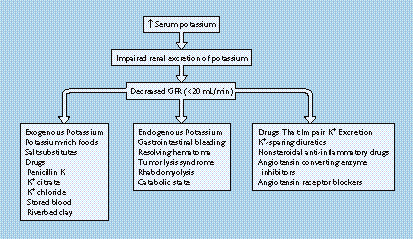
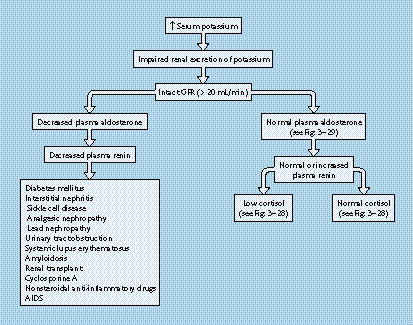 FIGURE 3-24
FIGURE 3-24
 Disorders of Water, Electrolytes, and Acid-Base
FIGURE 3-26
Disorders of Water, Electrolytes, and Acid-Base
FIGURE 3-26
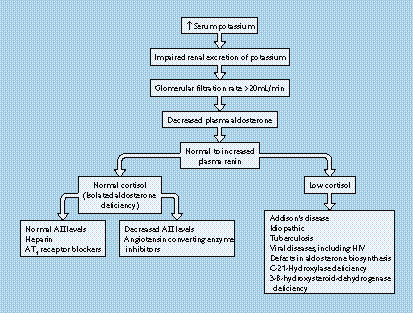
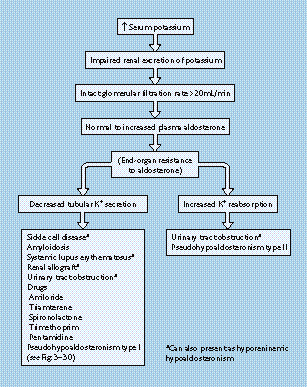 FIGURE 3-28
FIGURE 3-28