La spécificité du tadalafil est liée à sa longue demi-vie, permettant une action qui excède largement celle des autres inhibiteurs de PDE5. L’absorption digestive est complète, avec un pic plasmatique atteint en 2 heures environ. Le métabolisme est réalisé via CYP3A4, produisant des métabolites inactifs éliminés principalement dans les fèces. La sélectivité enzymatique est élevée, réduisant les effets indésirables extra-caverneux. Les réactions indésirables fréquentes incluent céphalées, bouffées vasomotrices et troubles digestifs légers. L’activité pharmacologique est stable, indépendamment de l’ingestion d’aliments. Dans les comparaisons de longue durée, acheter cialis pas cher est mentionné en relation avec les études portant sur la persistance d’efficacité et la constance de la cinétique plasmatique.
Childneuropsych-bg.com
Special Article Practice parameter: Steroids, acyclovir, and surgery for Bell’s palsy (an evidence-based review) Report of the Quality Standards Subcommittee of the American Academy of Neurology
Patrick M. Grogan, MD; and Gary S. Gronseth, MD
Article abstract—Objective: To determine the effectiveness of steroids, acyclovir, and surgical facial nerve decompression in Bell’s palsy. Methods: The authors identified articles by searching MEDLINE and selected those that prospectively compared outcomes in patients treated with steroids, acyclovir, or surgery with patients not receiving these modalities. The authors graded the quality of each study (class I to IV) using a standard classification-of-evidence scheme. They compared the proportion of patients recovering facial function in the treated group to the proportion of patients recovering facial function in the control group. Results: The authors identified no adequately powered class I studies for any treatment modality. The pooled results of two class I and two class II studies showed significantly better facial outcomes in steroid-treated patients compared with non–steroid-treated patients (relative rate good outcome 1.16, 95% CI 1.05 to 1.29). One class II study demonstrated a significant benefit from acyclovir in combination with prednisone compared with prednisone alone (relative rate good outcome 1.22, 95% CI 1.02 to 1.45). All studies describing outcomes in patients treated with facial nerve decompression were graded as class IV. Conclusion: For patients with Bell’s palsy, a benefit from steroids, acyclovir, or facial nerve decompression has not been definitively established. However, available evidence suggests that steroids are probably effective and acyclovir (combined with prednisone) is possibly effective in improving facial functional outcomes. There is insufficient evidence to make recommendations regarding surgical facial nerve decompression for Bell’s palsy. Well-designed studies of the effectiveness of treatments for Bell’s palsy are still needed.
The Quality Standards Subcommittee of the Ameri-
achieve near normal function.3 The disease is com-
can Academy of Neurology is charged with develop-
mon, with an annual incidence of 20 per 100,000.
Thus, despite its good prognosis, Bell’s palsy leaves
diagnostic procedures, treatment modalities, and
more than 8,000 people in the United States each
clinical disorders. The selection of topics for which
year with permanent, potentially disfiguring facial
practice parameters are developed is based on preva-
lence, frequency of use, economic impact, member-
Commonly employed, noncontroversial treatment
ship involvement, controversy, urgency, external
modalities for Bell’s palsy include eye patching and
constraints, and resources required. This report ad-
lubrication to protect the cornea.4 Controversy re-
dresses the effectiveness of controversial therapies
mains regarding the effectiveness of commonly used
pharmacologic therapies—steroids and acyclovir—as
Bell’s palsy is an acute, peripheral facial paresis of
well as surgical facial nerve decompression.
unknown cause.1 Usually, the diagnosis is estab-
Although the etiology of Bell’s palsy remains un-
lished without difficulty in patients presenting with
clear, there are reasons to believe steroids, acyclovir,
unexplained unilateral isolated facial weakness.2
or facial nerve decompression might improve out-
Most patients with Bell’s palsy recover without
comes in patients with this disorder. Bell’s palsy
treatment—71% achieve complete recovery, 84%
may result from inflammation and subsequent me-
Approved by the Quality Standards Subcommittee on July 29, 2000. Approved by the Practice Committee on August 5, 2000. Approved by the AAN Board ofDirectors on October 7, 2000.
Received July 21, 2000. Accepted in final form February 3, 2001.
Address correspondence and reprint requests to the American Academy of Neurology, 1080 Montreal Avenue, St. Paul, MN 55116.
Copyright 2001 by AAN Enterprises, Inc.
chanical compression5 of the facial nerve in the tem-
plete facial function. We also calculated the 95% CI
poral bone, possibly initiated by the herpes simplex
virus.6 Steroids might reduce facial nerve inflamma-
In studies using the House and Brackmann facial
tion, and surgery might relieve facial nerve compres-
function scoring system,7 we considered an outcome
sion, whereas acyclovir might treat the putative
of grade I or II a good recovery. When comparing the
proportion of patients recovering complete facial
To determine if steroids, acyclovir, and surgical
function, we considered an outcome of grade I a com-
facial nerve decompression are effective in improving
plete recovery. In studies using the Adour/Swanson
facial functional outcomes in Bell’s palsy, we performed
grading scale,8 we considered a facial paralysis re-
a systematic review and analysis of the literature.
covery profile (FPRP) of greater than seven and a
Based on this review, we propose recommendations
recovery index (FPRI) of greater than five a good
recovery. We considered an FPRP of 10 and an FPRIof 10 a complete recovery. Process.
Identification and selection of studies.
When necessary to improve the precision of the
We searched the National Library of Medicine’s
measured RR, we pooled the results from different
MEDLINE database from 1966 to June 2000. Three
studies using general variance-based meta-analytic
searches were performed in which we combined the
techniques.9 To minimize the risk of bias in the re-
term “facial paralysis or Bell’s palsy” with “pred-
sulting summary estimate of effect, we pooled stud-
nisone or prednisolone or hydrocortisone,” “acyclo-
ies with the lowest risk of bias first, adding studies
vir,” and “surgery.” We subsequently screened the
with a higher risk of bias only when necessary to
resultant articles and their references for those stud-
ies that compared outcomes in prospectively assem-
bled Bell’s palsy patients treated with steroids,
grade of class III or better were considered in the
acyclovir, or surgery to concurrent patients not
formulation of the recommendations. We formulated
practice recommendations after considering the esti-
mated effect sizes, the significance of the effect, and
sign characteristics were extracted from the identi-
the consistency of the effect between studies.
To account for the quality of evidence, we deter-
mined a strength-of-recommendation level for each
recommendation using the scheme in Appendix 2.
Age, sex, severity of palsy, and duration of palsy
We determined the strength of recommendation
based on the number and quality of studies available
Medication regimen used or decompression proce-
to derive the estimate of effect. Thus, for example, an
intervention demonstrating a consistent and signifi-
cant benefit in two class I studies would earn a level
Percentage of patients completing the study.
“A” recommendation. We planned to recommend
Method of facial function outcome assessment, in-
such an intervention as established as effective. An
intervention demonstrating a consistent and signifi-
We graded the quality of the evidence provided by
cant effect in two class II studies would earn a level
each study (class I, II, III, IV) using the classification-
“B” recommendation and would be recommended as
of-evidence scheme in Appendix 1. In this scheme, class
probably effective. Similarly, an intervention demon-
I studies are judged to have a low risk of bias and class
strating a consistent and significant benefit in two
IV studies are judged to have a high risk of bias. Stud-
class III studies would earn a level “C” recommenda-
ies were graded independently by each author. Differ-
tion. We planned to recommend such an intervention
ences were resolved after discussion.
using two-by-two tables, we compared the proportion
Analysis. In patients with Bell’s palsy, do steroids
of patients recovering good facial function in the
improve facial functional outcomes?
treated group to the proportion of patients recover-
identified 230 articles that described steroid use for
ing good facial function in the control group by calcu-
the treatment of Bell’s palsy. Nine8,10-17 of these stud-
lating the relative rate (RR) by means of the
ies prospectively compared outcomes in patients
treated with oral steroids to concurrent patients whowere not treated with steroids. The characteristics of
RR ϭ ͓A/͑A ϩ C͔͒/͓B/͑B ϩ D͔͒.
these studies are listed in table 1. Recovery Good Poor
tients meeting standard diagnostic criteria for Bell’s
Treated A
palsy were allocated to treatment with steroids or
placebo. Most studies limited enrollment to adults. One study17 enrolled children only. The proportion of
In separate analyses, we calculated the RR at
patients with severe facial weakness in each study
which patients in the treated group recovered com-
varied considerably (0 to 91%). The time allowed
April (1 of 2) 2001 Table 1 Design characteristics and outcomes in controlled studies of patients with Bell’s palsy treated with steroids
Severity, Duration, Follow-up, Completion
Completion rate: percentage of subjects followed to study completion; severity: percentage of patients with complete palsy; duration: maximum duration of palsy before starting ste-
Rx ϭ medication; CI ϭ 95% confidence interval; NH ϭ natural history, percentage of non–steroid-treated patients attaining a good outcome; RR ϭ relative rate of steroid-treated
patients attaining outcome compared to non–steroid-treated patients; NS ϭ not stated.
from symptom onset to treatment allocation also var-
less likely to have hypertension. Because hyperten-
ied widely between studies (2 to 14 days).
sion is an independent risk factor for poor facial out-
With the exception of one study11 that used hydro-
comes,1 a spurious association between steroids and
cortisone, authors used oral prednisone or pred-
improved facial outcomes may have resulted.
nisolone. Authors from another study12 did not
Because of unmasked, nonindependent outcome
specify the corticosteroid used, but we assumed it
assessments, as well as other methodologic flaws,
was prednisone because the dosage was similar to
we graded the evidence from four studies8,15-17 as
other studies using this medication. Multiple dosage
regimens of oral steroids were used. The most com-
monly reported regimen was 1 mg/kg of oral pred-
or complete recovery in steroid-treated patients rela-
nisone, up to 70 mg per day, split into twice-daily
tive to untreated patients. Although included in the
dosing. The starting dose was continued for 6 days,
table for completeness, because of a high risk of bias,
then tapered off over a subsequent 4 days. Outcomes
the results of class IV studies will not be discussed
in most studies were determined after 6 or more
The results of the five class I, II, and III studies
We graded the evidence from two studies10,11 as
were mixed. The two class I studies10,11 and one class
class I. In both, patients were randomly allocated to
II study12 did not show significantly better outcomes
steroids or placebo, no patients were lost to follow-
in steroid-treated patients. However, these studies
up, and outcomes were assessed in a masked
were insufficiently powered to exclude a clinically
important effect from steroids. One class II13 and one
We graded the evidence from two studies as class
class III14 study demonstrated significantly better
II.12,13 One class II study12 employed a quasi-
outcomes in the steroid-treated patients. In these
randomization technique (every other patient). This
studies, patients with Bell’s palsy were 1.2 times as
may have unmasked treatment allocation. We
likely to attain good facial functional recovery as un-
graded a second study13 as class II because 29% of
treated patients. No study showed significantly
worse facial functional outcomes in patients treated
We graded one14 nonrandomized, unmatched, con-
with steroids. Four of five of the studies demon-
trolled study with masked outcome assessments as
strated a trend for better outcomes in the steroid-
class III. In this study, there were important con-
founding baseline differences between steroid-
No study showed a significant difference in the
time to recovery between steroid-treated patients
example, steroid-treated patients in this study were
and controls. One class I study10 reported a median
April (1 of 2) 2001
time to recovery of 45 days in both steroid-treatedand untreated patients. One class II13 and one class Istudy11 reported a trend for steroid-treated patientsto recover faster than did control patients, but thedifferences were not significant. The average numberof days to recovery were 51 vs 69 and 63 vs 69,respectively.
None of the class I, II, or III studies described a
significant decrease in the frequency of autonomicsynkinesis (e.g., “crocodile tears”) in patients treatedwith steroids.
Some authors have suggested that steroids work
best in patients with Bell’s palsy if started early.18The articles reviewed provided little evidence to sup-
Figure. Relative rates of good outcomes (rectangles) with
port or refute this assertion. Most of the patients
95% CI (vertical lines) in steroid-treated patients com-
enrolled in these studies were treated within 1 week
pared with non–steroid-treated patients. Pooled relativerate of class I and II studies is indicated by vertical
of onset of facial paralysis. The class III study14
showed a nonsignificant trend of more benefit in pa-tients who received steroids early (by day 1: RR 1.25;by day 2: RR 1.19; by day 3: RR 1.12).
However, the RR derived from this class III study
mation regarding the response of Bell’s palsy patient
was also the most prone to bias. The nonrandom
subgroups, such as patients with diabetes mellitus,
treatment allocation employed in this study resulted
hypertension, or recurrent facial palsy. Thus, we
in prognostically important differences between
were unable to determine if the association between
steroid-treated and non–steroid-treated patients.
steroid treatment and facial outcomes was different
These confounding differences may have resulted in
a spurious association between steroids and im-
Bell’s palsy patients with incomplete facial paral-
ysis have excellent outcomes regardless of therapy.3
To increase the precision of the measured RR
Thus, some have suggested that patients with com-
while minimizing the risk of bias, we statistically
plete facial palsy benefit most from steroids.15 The
pooled the rates from the two class I studies. The
studies reviewed here provided little evidence rela-
pooled result from these studies10,11 did not demon-
tive to this issue. In a two-way analysis of variance
strate a significant benefit from steroids (RR 1.01).
of time to recovery, one class II study13 found no
However, the 95% CI of the combined RR was still
interaction between treatment and the severity of
too wide (0.80 to 1.27). The pooled result was insuffi-
facial weakness at the onset of treatment.
To further increase precision, we combined the RR
roid side effects. Side effects occurred in 1 to 4% of
of good facial recovery from the class I and class II
treated patients. These side effects, in descending
studies. While increasing the precision of the derived
order of frequency, were dyspepsia, loss of blood
RR of recovery, including the class II studies in-
sugar control, recurrent duodenal ulcers, mood
creased the risk of bias in the summary estimate of
swings, and acute psychosis. All effects resolved
effect. The pooled RR from the two class I and two
class II studies demonstrated a significant associa-
tion between steroids and good outcomes (RR 1.16,
in steroid-treated patients relative to non–steroid-
95% CI 1.05 to 1.29, vertical diamond in the figure).
treated patients extracted from each study are plot-
Thus, assuming 80% of patients with Bell’s palsy
ted in the figure. The measured RR are ordered, left
attain good facial outcomes without steroid treat-
to right, by class of evidence. The 95% CI are repre-
ment, an additional 14% might attain good outcomes
if treated with steroids. The pooled effect from the
None of the studies reviewed were conclusive. The
class I and II studies was homogenous (p ϭ 0.59)
RR with the lowest risk of bias came from the class I
with overlapping CI. This suggests that the differ-
studies.10,11 Both employed random, masked method-
ences in the study results were potentially related to
ologies. Although at low risk for bias, the measured
RR from these class I studies were the least precise.
This is indicated in the figure by the tall CI. These
ciently powered class I studies, we conclude that a
class I studies enrolled too few patients to defini-
benefit of steroids in Bell’s palsy has not been defin-
tively exclude an important effect (either benefit or
itively established. However, the available evidence
supports a level “B” recommendation using the
A more precise measure of the effect of steroids
scheme in Appendix 2. Thus, based on the pooled
came from the single class III study.14 In this study,
result of class I and class II studies and a relatively
authors enrolled the largest number of patients.
benign side effect profile, we conclude that steroids
April (1 of 2) 2001 Table 2 Design characteristics and outcomes in controlled studies of patients with Bell’s palsy treated with acyclovir
Completion rate: percentage of subjects followed to study completion; severity: percentage of patients with complete palsy; duration: maximum duration of palsy before starting ste-
Rx ϭ medication; CI ϭ 95% confidence; NH ϭ natural history, percentage of non–acyclovir-treated patients attaining a good outcome; RR ϭ relative rate of acyclovir-treated pa-
tients attaining outcome compared to non–acyclovir-treated patients; NS ϭ not stated.
are safe and probably effective in improving facial
mine if the side effects reported were secondary to
functional outcomes in patients with Bell’s palsy. In patients with Bell’s palsy, does acyclovir im-
studies, we conclude that a benefit of acyclovir in
egy identified 92 articles that described acyclovir use
Bell’s palsy has not been definitively established.
for the treatment of Bell’s palsy. Three19-21 of these
However, the available evidence supports a level “C”
studies prospectively compared outcomes in treated
recommendation using the scheme in Appendix 2.
patients with those not treated with acyclovir. Study
Thus, based on the result of a single class II study
characteristics and outcomes of these studies are
and a relatively benign side effect profile, we con-
clude that acyclovir (combined with prednisone) is
safe and possibly effective in improving facial func-
tients meeting standard diagnostic criteria for Bell’s
tional outcomes in patients with Bell’s palsy.
palsy were allocated to treatment with acyclovir or
In patients with Bell’s palsy, does facial nerve de-
prednisone. Two studies19,21 compared the effect of a
compression improve facial functional outcomes?
combination of acyclovir and prednisone vs pred-
We found 104 articles describing surgical facial
nisone alone. One study20 compared acyclovir alone
nerve decompression in patients with Bell’s palsy.
to prednisone alone. The dose of acyclovir varied be-
Four12,22-25 of these studies prospectively compared
tween studies from 1,000 mg a day for 5 days to
outcomes in patients treated with surgery to those
2,400 mg a day for 10 days. Outcomes were mea-
not treated. The characteristics and outcomes of
sured after 3 to 12 months of follow-up.
these studies are listed in table 3.
One study19 employed randomized treatment allo-
cation and masked outcome assessments. However,
meeting standard diagnostic criteria for Bell’s palsy
17% of enrolled patients were lost to follow-up. For
were allocated to treatment with facial nerve decom-
this reason, we graded evidence from this study as
pression or medical therapy. The majority of patients
class II. Because of unmasked, nonindependent out-
in each study had complete facial paralysis and for
come assessments, as well as other methodologic
this reason had poorer prognoses.1 Most had been
flaws, the evidence from the two remaining stud-
treated with steroids. Authors reported varied surgi-
cal approaches. Outcomes were measured after 6 to
or complete recovery in acyclovir-treated patients
Patients were not randomly allocated to surgical
relative to patients treated with prednisone alone.
and nonsurgical groups in any study. Additionally,
The single class II study19 demonstrated a signifi-
no study described masked or independent assess-
cant benefit of acyclovir. In this study, patients
ment of facial functional outcomes. For these rea-
treated with acyclovir and prednisone were 1.22
sons, the evidence from all of these studies was
times more likely to attain good outcomes than pa-
tients treated with prednisone alone (95% CI 1.02 to
1.45). Thus, assuming 80% of patients with Bell’s
or complete recovery in patients undergoing facial
palsy attain good outcomes on steroids alone, an ad-
nerve decompression relative to nonsurgical patients
ditional 18% might attain good outcomes if treated
from each of the class IV studies. Only one study22
demonstrated a significant association between sur-
ture of side effects in the acyclovir trials were similar
to those with steroids.19-21 It was impossible to deter-
was the most common serious side effect from facial
April (1 of 2) 2001 Table 3 Design characteristics and outcomes in controlled studies of patients with Bell’s palsy treated with facial nerve decompression
Severity, Duration, Follow-up, Completion
Completion rate: percentage of subjects followed to study completion; severity: percentage of patients with complete palsy; duration: maximum duration of palsy before starting ste-
CI ϭ 95% confidence interval; NH ϭ natural history, percentage of nonsurgical patients attaining a good outcome; RR ϭ relative rate of surgically treated patients attaining out-
come compared to non–surgically treated patients; NS ϭ not stated.
nerve decompression reported in these articles. The
Masked, standardized outcome assessments, in-
study published in 198212 reported deafness in 15%
of patients undergoing facial nerve decompression.
Sufficient power to detect important differences
More recent trials report much lower complication
Subgroup analyses to detect interactions between
treatment, severity of paralysis, duration of palsy
scribing facial outcomes in surgically treated Bell’s
before initiation of therapy, and patient characteris-
palsy patients was too high to support evidence-
tics such as the diabetes mellitus, hypertension, and
based conclusions. Additionally, serious complica-
tions, including permanent hearing loss, werereported from surgical facial nerve decompression. Disclaimer.
For these reasons, we were unable to develop
educational service of the American Academy of
evidence-based recommendations for the use of facial
Neurology. It is based on an assessment of current
nerve decompression in patients with Bell’s palsy.
scientific and clinical information. It is not intendedto include all possible proper methods of care for a
Practice recommendations.
particular neurologic problem or all legitimate crite-
ria for choosing to use a specific procedure. Neither
Early treatment with oral steroids is recom-
is it intended to exclude any reasonable alternative
mended as probably effective to improve facial func-
methodologies. The AAN recognizes that specific
care decisions are the prerogative of the patient and
Early treatment with acyclovir in combination
the physician caring for the patient, based on all of
with prednisone is recommended as possibly effective
to improve facial functional outcomes (Level C).
There is insufficient evidence to make recommen-
Acknowledgment
dations regarding the use of facial nerve decompres-sion to improve facial functional outcomes (Level U).
The authors thank the members of the Quality Standards Sub-committee of the American Academy of Neurology, Wendy Ed-lund, the AAN Manager, Clinical Practice Guidelines, and Alison
Recommendations for future research.
Nakashima, AAN Administrator, Clinical Practice Guidelines, for
preceding recommendations are based on the best
their time, expertise, and efforts in developing this document. Theauthors also thank Rollin J. Hawley, MD, FACP, Viliam J. Fur-
available evidence regarding the effectiveness of ste-
dik, MD, and William Bishop, MD, for their role in initiating this
roids, acyclovir, and facial nerve decompression for
Bell’s palsy. All of the studies reviewed had flaws,including insufficient statistical power and bias-
Appendix 1
prone methodologies that preclude definitive conclu-
Definitions for classification of evidence
sions. Definitive studies of the effectiveness of these
Class I. Evidence provided by a randomized, controlled clinical
modalities are still needed. Investigators contem-
trial (RCT) with masked outcome assessment in a representative
plating such studies should carefully weigh the risk
population. The following are required: a) primary outcomes are
of the intervention relative to its potential benefit.
clearly defined; b) exclusion and inclusion criteria are clearly stat-
The design of such studies should include the following:
ed; c) adequate accounting of dropouts and crossovers with num-bers sufficiently low to have minimal potential for bias; and d)
Random allocation to treatment groups.
relevant baseline characteristics are substantially equivalent
Complete follow-up of enrolled patients. April (1 of 2) 2001 Class II. Evidence provided by a prospective matched group
geniculate ganglion of a patient with Bell’s palsy. Ann Otol
cohort study in a representative population with masked outcome
assessment that meets a through d above or an RCT that lacks
7. House JW, Brackmann DE. Facial nerve grading system. Oto-
laryngol Head Neck Surg 1985;93:146 –147. Class III. All other controlled trials (including well-defined
8. Adour KK, Wingerd J, Bell DN, Manning JJ, Hurley JP. Pred-
natural history controls or patients serving as their own controls)
nisone treatment for idiopathic facial paralysis (Bell’s palsy).
in a representative population where outcome assessment is inde-
9. Petitti DB. Statistical methods in meta-analysis. In: Petitti
Class IV. Evidence from studies not assessing outcomes inde-
DB. Meta-analysis, decision analysis and cost-effectiveness
pendent of treatment, uncontrolled studies, case series, case re-
analysis. New York, NY: Oxford University Press, 1994;90 –
10. May M, Wette R, Hardin WB, Sullivan J. The use of steroids
Appendix 2
in Bell’s palsy: a prospective controlled study. Laryngoscope
Definitions for strength of recommendations
11. Taverner D. Cortisone treatment of Bell’s palsy. Lancet 1954;
Level A. Established as effective, ineffective, or harmful for the
given condition in the specified population. Usually, an “A” recom-
12. Brown JS. Bell’s palsy: a 5-year review of 174 consecutive
mendation requires that the pooled result from two or more dis-
cases: an attempted double blind study. Laryngoscope 1982;
tinct class I studies demonstrates a consistent, significant, and
13. Austin JR, Peskind SP, Austin SG, Rice DH. Idiopathic facial
Level B. Probably effective, ineffective, or harmful for the given
nerve paralysis: a randomized double blind controlled study of
condition in the specified population. Usually, a “B” recommenda-
placebo versus prednisone. Laryngoscope 1993;103:1326 –1333.
tion requires that a single class I study demonstrates a significant
14. Shafshak TS, Essa AY, Bakey FA. The possible contributing
and important effect or the pooled result from two or more distinct
factors for the success of steroid therapy in Bell’s palsy: a
class II studies demonstrates a consistent, significant, and impor-tant effect.
clinical and electrophysiological study. J Laryngol Otol 1994;
Level C. Possibly effective, ineffective, or harmful for the given
condition in the specified population. Usually, a “C” recommenda-
15. Wolf SM, Wagner JH, Davidson S, Forsythe A. Treatment of
tion requires that a single class II study demonstrates a signifi-
Bell palsy with prednisone: a prospective randomized study.
cant and important effect or the pooled result of two or more
distinct class III studies demonstrates a consistent, significant,
16. Abraham–Inpijn L, Oosting J, Hart AA. Bell’s palsy: factors
affecting the prognosis in 200 patients with reference to hy-
Level U. Data are inadequate or conflicting. Given current
pertension and diabetes mellitus. Clin Otolaryngol 1987;12:
knowledge, treatment is unproven and an evidence-based recom-
17. Unuvar E, Oguz F, Sidal M, Kilic A. Corticosteroid treatment
of childhood Bell’s palsy. Pediatr Neurol 1999;21:814 – 816. Appendix 3
18. May MM, Schlaepfer WM. Bell’s palsy and the chorda tym-
pani nerve: a clinical and electron microscopic study. Laryngo-
Quality Standards Subcommittee Members: Gary Franklin,
MD, MPH (Co-Chair); Catherine Zahn, MD (Co-Chair); Milton
19. Adour KK, Ruboyianes JM, Von Doersten PG, et al. Bell’s
Alter, MD, PhD; Stephen Ashwal, MD; John Calverley, MD; Rich-
palsy treatment with acyclovir and prednisone compared with
ard M. Dubinsky, MD; Jacqueline French, MD; Michael Glantz,
prednisone alone: a double blind, randomized, controlled trial.
MD; Gary Gronseth, MD; Deborah Hirtz, MD; Robert G. Miller,
Ann Otol Rhinol Laryngol 1996;105:371–378.
MD; James Stevens, MD; and William Weiner, MD.
20. De Diego JI, Prim MP, De Sarria MJ, Madero R, Gavilan J.
Idiopathic facial paralysis: a randomized, prospective, and
References
controlled study using single-dose prednisone versus acyclovirthree times daily. Laryngoscope 1998;108:573–575.
1. Hauser WA, Karnes WE, Annis J, Kurland LT. Incidence and
prognosis of Bell’s palsy in the population of Rochester, Min-
21. Ramos MA, De Miguel Martinez I, Martin Sanchez AM, Go-
nesota. Mayo Clin Proc 1971;46:258 –264.
mez Gonzalez JL, Martin Galan A. Incorporacion del aciclovir
2. Katusic SK, Beard CM, Wiederholt WC, et al. Incidence, clin-
en el tratamiento de la paralisis periferica. Un estudio en 45
ical features, and prognosis in Bell’s palsy. Ann Neurol 1986;
casos. Acta Otorrinolaringol Esp 1992;43:117–120.
22. Gantz BJ, Rubinstein JT, Gidley P, Woodworth GG. Surgical
3. Peitersen E. The natural history of Bell’s palsy. Am J Otol
management of Bell’s palsy. Laryngoscope 1999;109:1177–1188.
23. May MM, Taylor FH. Bell’s palsy: surgery based upon prog-
4. Hughes GB. Practical management of Bell’s palsy. Otolaryn-
nostic indicators and results. Laryngoscope 1981;91:2092–2105.
gol Head Neck Surg 1990;102:658 – 663.
24. May MM, Klein SR, Taylor FH. Idiopathic (Bell’s) facial palsy:
5. Hilger J. The nature of Bell’s palsy. Laryngoscope 1949;59:
natural history defies steroid or surgical treatment. Laryngo-
6. Burgess RC, Michaels L, Bale JF, Smith RJ. Polymerase chain
25. Fisch U. Surgery for Bell’s palsy. Arch Otolaryngol 1981;107:
reaction amplification of Herpes simplex viral DNA from the
April (1 of 2) 2001
MATERIAL SAFETY DATA SHEET Date Printed: 10/19/2006 Date Updated: 05/25/2006 Version 1.8 Section 1 - Product and Company Information Product Name AMPICILLIN SODIUM SALT Product Number APAM-0001 Brand SIAL Company Sigma-Aldrich Address 3050 Spruce Street SAINT LOUIS MO 63103 US Technical Phone: 800-325-5832 Fax: 800-325-5052 Emergency Phone: 314-776-6555 Section 2 - Composition/Information on
HIV: Where Are We Now? Current Approvals State Approval Access Continuing Education, Inc. is a Florida-approved provider of continuing education for nurses, provider # 50-7628. Continuing Education Credit This course has been awarded 2.0 contact hours for nurses by Access Continuing Education, Inc. an approved provider of continuing nursing education by the Vermont State Nur
 Special Article
Special Article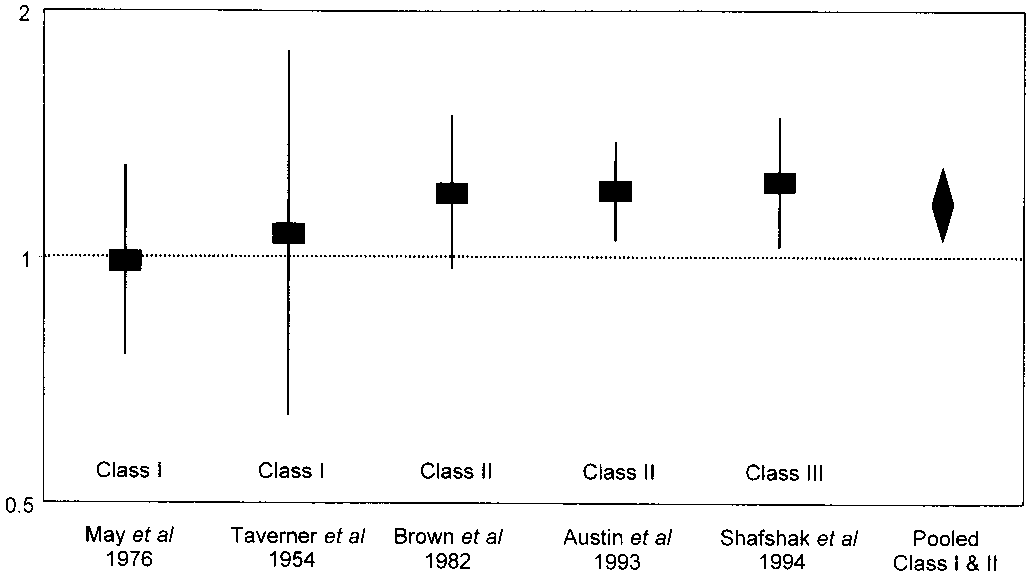 time to recovery of 45 days in both steroid-treatedand untreated patients. One class II13 and one class Istudy11 reported a trend for steroid-treated patientsto recover faster than did control patients, but thedifferences were not significant. The average numberof days to recovery were 51 vs 69 and 63 vs 69,respectively.
time to recovery of 45 days in both steroid-treatedand untreated patients. One class II13 and one class Istudy11 reported a trend for steroid-treated patientsto recover faster than did control patients, but thedifferences were not significant. The average numberof days to recovery were 51 vs 69 and 63 vs 69,respectively.